

This is a preprint.
SARS-CoV-2 shedding and evolution in immunocompromised hosts during the Omicron period: a multicenter prospective analysis
- PMID: 37662226
- PMCID: PMC10473782
- DOI: 10.1101/2023.08.22.23294416
SARS-CoV-2 shedding and evolution in immunocompromised hosts during the Omicron period: a multicenter prospective analysis
Update in
-
SARS-CoV-2 shedding and evolution in patients who were immunocompromised during the omicron period: a multicentre, prospective analysis.Lancet Microbe. 2024 Mar;5(3):e235-e246. doi: 10.1016/S2666-5247(23)00336-1. Epub 2024 Jan 26. Lancet Microbe. 2024. PMID: 38286131 Free PMC article.
Abstract
Background: Prolonged SARS-CoV-2 infections in immunocompromised hosts may predict or source the emergence of highly mutated variants. The types of immunosuppression placing patients at highest risk for prolonged infection and associated intrahost viral evolution remain unclear.
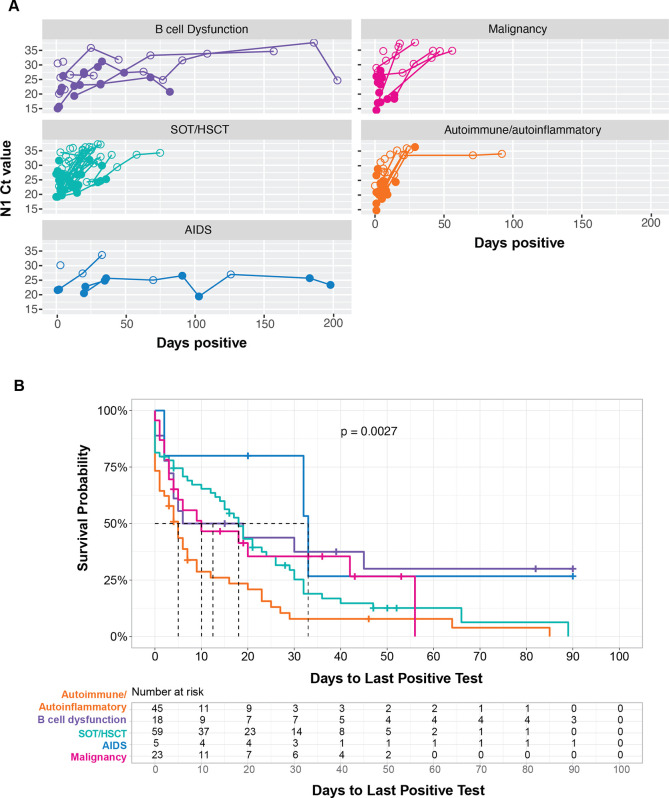
Methods: Adults aged ≥18 years were enrolled at 5 hospitals and followed from 4/11/2022 - 2/1/2023. Eligible patients were SARS-CoV-2-positive in the previous 14 days and had a moderate or severely immunocompromising condition or treatment. Nasal specimens were tested by rRT-PCR every 2-4 weeks until negative in consecutive specimens. Positive specimens underwent viral culture and whole genome sequencing. A Cox proportional hazards model was used to assess factors associated with duration of infection.
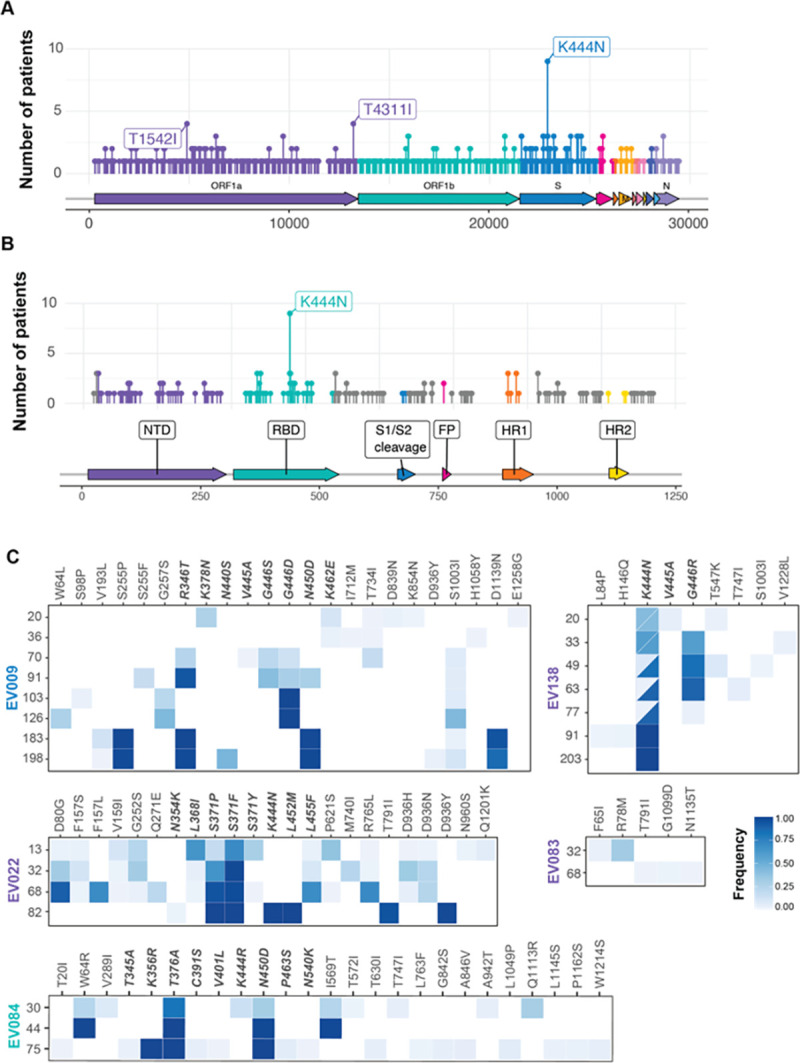
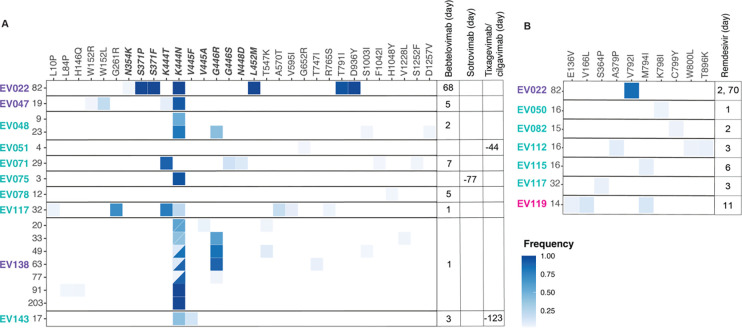
Results: We enrolled 150 patients with: B cell malignancy or anti-B cell therapy (n=18), solid organ or hematopoietic stem cell transplant (SOT/HSCT) (n=59), AIDS (n=5), non-B cell malignancy (n=23), and autoimmune/autoinflammatory conditions (n=45). Thirty-eight (25%) were rRT-PCR-positive and 12 (8%) were culture-positive ≥21 days after initial SARS-CoV-2 detection or illness onset. Patients with B cell dysfunction had longer duration of rRT-PCR-positivity compared to those with autoimmune/autoinflammatory conditions (aHR 0.32, 95% CI 0.15-0.64). Consensus (>50% frequency) spike mutations were identified in 5 individuals who were rRT-PCR-positive >56 days; 61% were in the receptor-binding domain (RBD). Mutations shared by multiple individuals were rare (<5%) in global circulation.
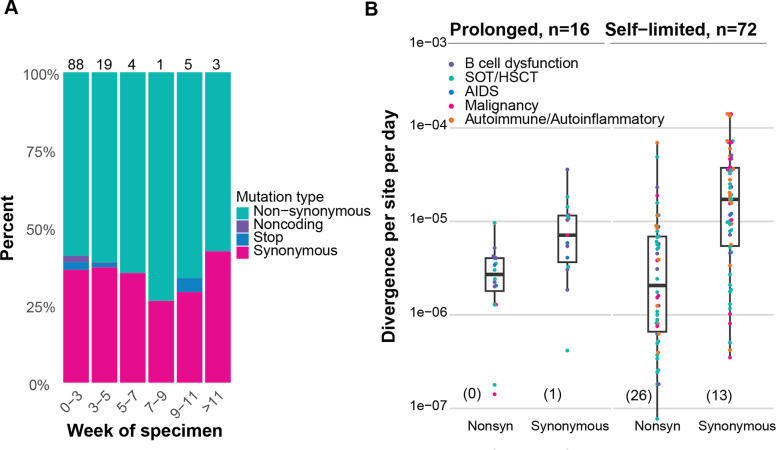
Conclusions: In this cohort, prolonged replication-competent Omicron SARS-CoV-2 infections were uncommon. Within-host evolutionary rates were similar across patients, but individuals with infections lasting >56 days accumulated spike mutations, which were distinct from those seen globally.
Keywords: COVID-19; SARS-CoV-2; evolution; immunocompromise; prolonged replication.
Conflict of interest statement
CONFLICTS OF INTEREST All authors have completed ICMJE disclosure forms (www.icmje.org/coi_disclosure.pdf). James Chappell reports receiving grants from NIH and DoD, outside the submitted work. Carlos Grijalva reports grants from NIH, CDC, AHRQ, FDA, Campbell Alliance/Syneos Health, consulting fees and participating on a DSMB for Merck, outside the submitted work. Anne Frosch reports a K08 award from NIH and participating on the Hennepin Health Research Institute Board of Directors, outside the submitted work. Natasha Halasa reports grants from Sanofi, Quidel, and Merck, outside the submitted work. Adam Lauring reports receiving grants from CDC, NIAID, Burroughs Wellcome Fund, Flu Lab, and consulting fees from Roche, outside the submitted work. Emily Martin reports receiving a grant from Merck, outside the submitted work.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous