

This is a preprint.
Preventing tuberculosis with community-based care in an HIV-endemic setting: a modeling analysis
- PMID: 37662260
- PMCID: PMC10473784
- DOI: 10.1101/2023.08.21.23294380
Preventing tuberculosis with community-based care in an HIV-endemic setting: a modeling analysis
Update in
-
Preventing tuberculosis with community-based care in an HIV-endemic setting: a modelling analysis.J Int AIDS Soc. 2024 Jun;27(6):e26272. doi: 10.1002/jia2.26272. J Int AIDS Soc. 2024. PMID: 38861426 Free PMC article.
Abstract
Introduction: Antiretroviral therapy (ART) and TB preventive treatment (TPT) both prevent tuberculosis (TB) disease and deaths among people living with HIV. Differentiated care models, including community-based care, can increase uptake of ART and TPT to prevent TB in settings with a high burden of HIV-associated TB, particularly among men.
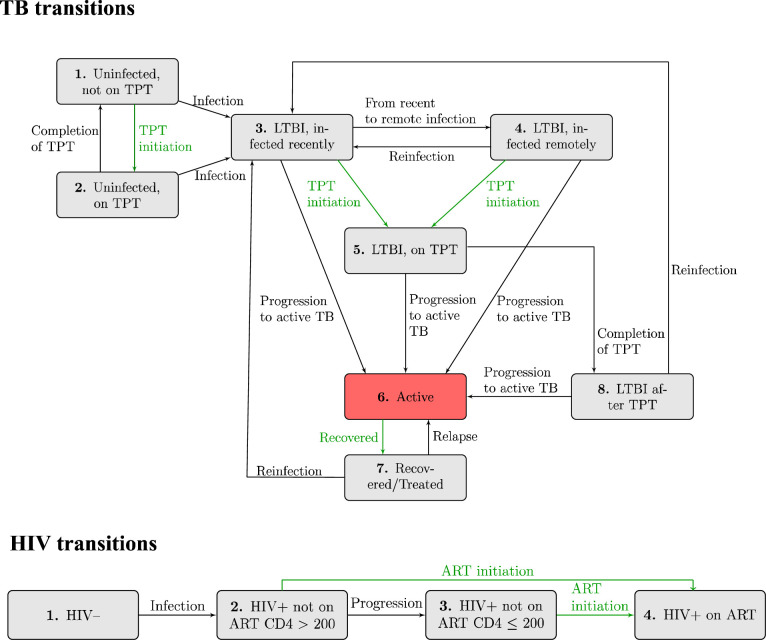
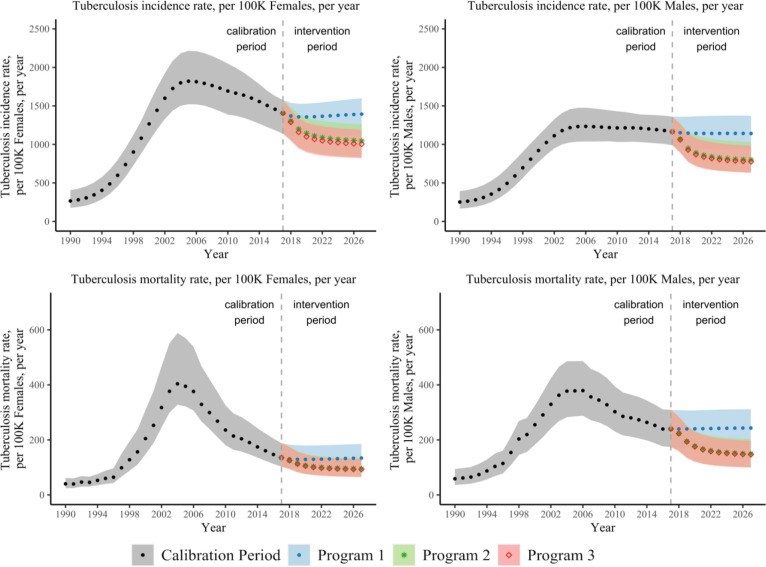
Methods: We developed a gender-stratified dynamic model of TB and HIV transmission and disease progression among 100,000 adults ages 15-59 in KwaZulu-Natal, South Africa. We drew model parameters from a community-based ART initiation and resupply trial in sub-Saharan Africa (Delivery Optimization for Antiretroviral Therapy, DO ART) and other scientific literature. We simulated the impacts of community-based ART and TPT care programs during 2018-2027, assuming that community-based ART and TPT care were scaled up to similar levels as in the DO ART trial (i.e., ART coverage increasing from 49% to 82% among men and from 69% to 83% among women) and sustained for ten years. We projected the number of TB cases, deaths, and disability-adjusted life years (DALYs) averted relative to standard, clinic-based care. We calculated program costs and incremental cost-effectiveness ratios from the provider perspective.
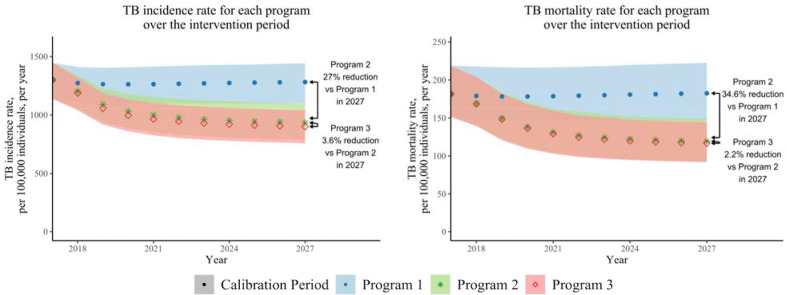
Results: If community-based ART care could be implemented with similar effectiveness to the DO ART trial, increased ART coverage could reduce TB incidence by 27.0% (range 21.3% - 34.1%) and TB mortality by 36.0% (range 26.9% - 43.8%) after ten years. Increasing both ART and TPT uptake through community-based ART with TPT care could reduce TB incidence by 29.7% (range 23.9% - 36.0%) and TB mortality by 36.0% (range 26.9% - 43.8%). Community-based ART with TPT care reduced gender disparities in TB mortality rates by reducing TB mortality among men by a projected 39.8% (range 32.2% - 46.3%) and by 30.9% (range 25.3% - 36.5%) among women. Over ten years, the mean cost per DALY averted by community-based ART with TPT care was $846 USD (range $709 - $1,012).
Conclusions: By substantially increasing coverage of ART and TPT, community-based care for people living with HIV could reduce TB incidence and mortality in settings with high burdens of HIV-associated TB and reduce TB gender disparities.
Keywords: Differentiated care; HIV epidemiology; TB; cost effectiveness; gender; modeling.
Conflict of interest statement
Competing interests The authors declare no competing interests.
Figures

References
-
- World Health Organization. Global Tuberculosis Report. 2022.
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, Raviglione MC, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med [Internet]. 2003. May 12;163(9):1009–21. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12742798 - PubMed
-
- Moyo S, Ismail F, Van der Walt M, Ismail N, Mkhondo N, Dlamini S, et al. Prevalence of bacteriologically confirmed pulmonary tuberculosis in South Africa, 2017–19: a multistage, cluster-based, cross-sectional survey. Lancet Infect Dis [Internet]. 2022. May 17; Available from: http://www.ncbi.nlm.nih.gov/pubmed/35594897 - PMC - PubMed
-
- Human Sciences Research Council. South African National HIV Prevalence, Incidence, Behaviour and Communication survey, 2017. Towards achieving the UNAIDS 90–90-90 targets. 2019. Oct.
-
- Ledesma JR, Ma J, Vongpradith A, Maddison ER, Novotney A, Biehl MH, et al. Global, regional, and national sex differences in the global burden of tuberculosis by HIV status, 1990–2019: results from the Global Burden of Disease Study 2019. Lancet Infect Dis [Internet]. 2021. Sep; Available from: https://linkinghub.elsevier.com/retrieve/pii/S1473309921004497 - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources