

Appearance of aseptic vascular grafts after endovascular aortic repair on [(18)F]fluorodeoxyglucose positron emission tomography/computed tomography
- PMID: 37662425
- PMCID: PMC10473915
- DOI: 10.4329/wjr.v15.i8.241
Appearance of aseptic vascular grafts after endovascular aortic repair on [(18)F]fluorodeoxyglucose positron emission tomography/computed tomography
Abstract
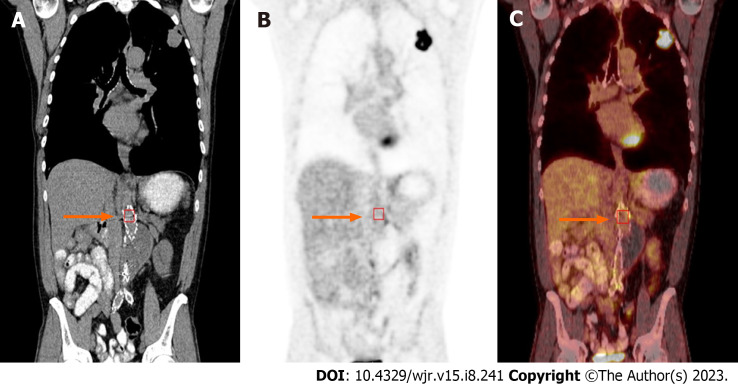
Background: Diagnosis of prosthetic vascular graft infection with [(18)F]fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) allows for early detection of functional changes associated with infection, based on increased glucose utilization by activated macrophages and granulocytes. Aseptic vascular grafts, like all foreign bodies, can stimulate an inflammatory response, which can present as increased activity on 18F-FDG PET/CT. Consequently, distinguishing aseptic inflammation from graft infection, though important, can be difficult. In the case of endovascular aneurysm repair (EVAR), a minimally invasive procedure involving the transfemoral insertion of an endoprosthetic stent graft, the normal postoperative appearance of these grafts on 18F-FDG PET/CT can vary over time, potentially confounding study interpretation.
Aim: To investigate the visual, semiquantitative, and temporal characteristics of aseptic vascular grafts in patients status post EVAR.
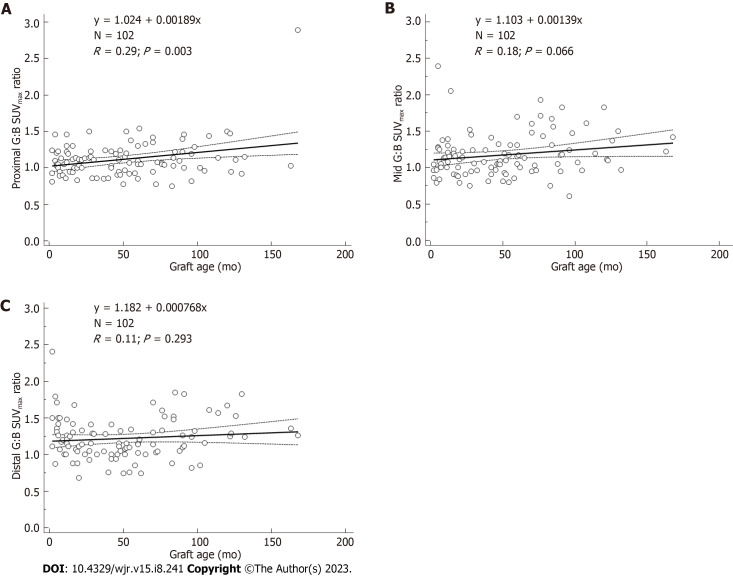
Methods: In this observational retrospective cohort study, patients with history of EVAR who underwent 18F-FDG PET/CT for indications other than infection were identified retrospectively. All patients were asymptomatic for graft infection - no abdominal pain, fever of unknown origin, sepsis, or leukocytosis - at the time of imaging and for ≥ 2 mo after each PET/CT. Imaging studies such as CT for each patient were also reviewed, and any patients with suspected or confirmed vascular graft infection were excluded. One hundred two scans performed on 43 patients (34 males; 9 females; age = 77 ± 8 years at the time of the final PET/CT) were retrospectively reviewed. All 43 patients had an abdominal aortic (AA) vascular graft, 40 patients had a right iliac (RI) limb graft, and 41 patients had a left iliac (LI) limb graft. Twenty-two patients had 1 PET/CT and 21 patients had from 2 to 9 PET/CTs. Grafts were imaged between 2 mo to 168 mo (about 14 years) post placement. Eight grafts were imaged within 6 mo of placement, including three that were imaged within three months of placement. The mean interval between graft placement and PET/CT for all 102 scans was 51 ± 39 mo. PET/CT data was reconstructed with region-of-interest analysis of proximal, mid and distal portions of the grafts and background ascending aorta. Maximum standardized uptake value (SUVmax) was recorded for each region. SUVmax-to-background uptake ratios (URs) were calculated. Visual assessment was performed using a 2-pattern grading scale: Diffuse (homogeneous uptake less than liver uptake) and focal (one or more areas of focal uptake in any part of the graft). Statistical analysis was performed.
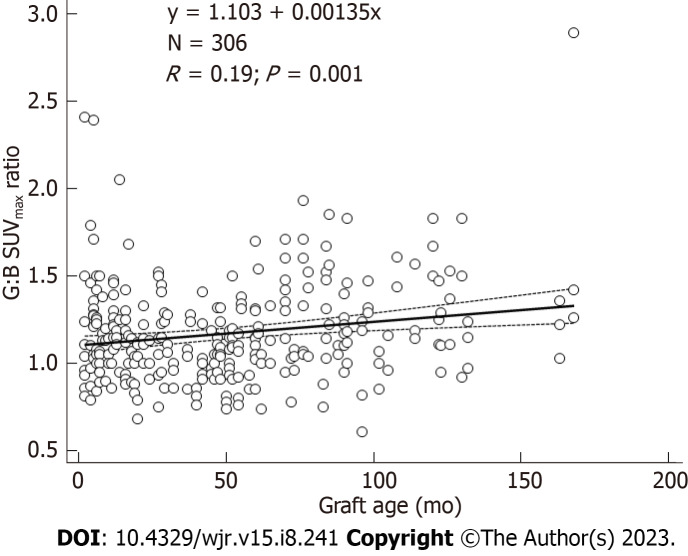
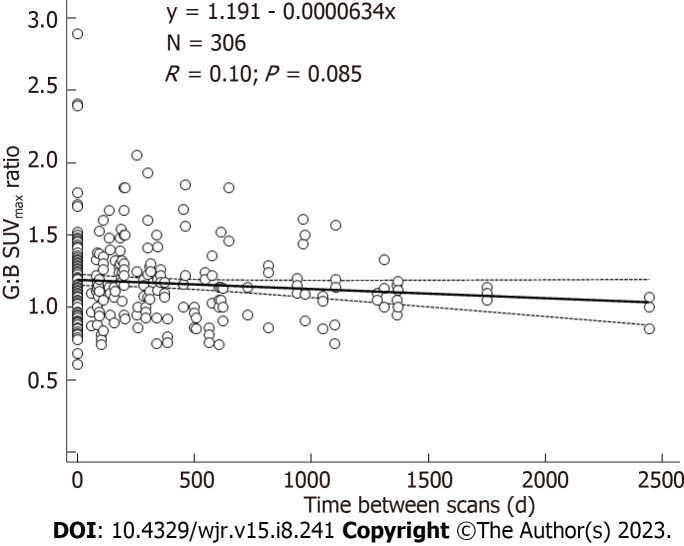
Results: In total, there were 306 AA grafts, 285 LI grafts, 282 RI grafts, and 306 ascending aorta background SUVmax measurements. For all 102 scans, mean SUVmax values for AA grafts were 2.8-3.0 along proximal, mid, and distal segments. Mean SUVmax values for LI grafts and RI grafts were 2.7-2.8. Mean SUVmax values for background were 2.5 ± 0.5. Mean URs were 1.1-1.2. Visual analysis of the scans reflected results of quantitative analysis. On visual inspection, 98% revealed diffuse, homogeneous 18F-FDG uptake less than liver. Graft URs and visual pattern categories were significantly associated for AA graft URs (F-ratio = 21.5, P < 0.001), LI graft URs (F-ratio = 20.4, P < 0.001), and RI graft URs (F-ratio = 30.4, P < 0.001). Thus, visual patterns of 18F-FDG uptake corresponded statistically significantly to semiquantitative URs. The age of grafts showing focal patterns was greater than grafts showing diffuse patterns, 87 ± 89 vs 50 ± 37 mo, respectively (P = 0.02). URs were significantly associated with graft age for AA grafts (r = 0.19, P = 0.001). URs were also significantly associated with graft age for LI grafts (r = 0.25, P < 0.0001), and RI grafts (r = 0.31, P < 0.001). Quartiles of similar numbers of graft (n = 25-27) grouped by graft age indicated that URs were significantly higher for 4th quartile vs 2nd quartile URs (F-ratio = 19.5, P < 0.001). When evaluating URs, graft SUVmax values within 10%-20% of the ascending aorta SUVmax is evident in aseptic grafts, except for grafts in the oldest quartiles. In this study, grafts in the oldest quartiles (> 7 years post EVAR) showed SUVmax up to 30% higher than the ascending aorta SUVmax.
Conclusion: Characteristics of an aseptic vascular stent graft in the aorta and iliac vessels on 18F-FDG PET/CT include graft SUVmax values within 10%-20% of the ascending aorta background SUVmax. The SUVmax of older aseptic grafts can be as much as 30% above background. The visual uptake pattern of diffuse, homogeneous uptake less than liver was seen in 98% of aseptic vascular grafts, making this pattern particularly reassuring for clinicians.
Keywords: Aseptic vascular grafts; Endovascular aortic repair; [(18)F]fluorodeoxyglucose positron emission tomography/computed tomography.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
Similar articles
-
Determining the Diagnostic Value of 18F-Fluorodeoxyglucose Positron Emission/Computed Tomography in Detecting Prosthetic Aortic Graft Infection.Ann Vasc Surg. 2018 Nov;53:78-85. doi: 10.1016/j.avsg.2018.04.028. Epub 2018 Aug 11. Ann Vasc Surg. 2018. PMID: 30012456
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
The relevance of 18F-fluorodeoxyglucose positron emission tomography/computed tomography imaging in diagnosing prosthetic graft infections post cardiac and proximal thoracic aortic surgery.Interact Cardiovasc Thorac Surg. 2015 Oct;21(4):450-8. doi: 10.1093/icvts/ivv178. Epub 2015 Jul 13. Interact Cardiovasc Thorac Surg. 2015. PMID: 26174118
-
A systematic review and meta-analysis of 18F-fluoro-d-deoxyglucose positron emission tomography interpretation methods in vascular graft and endograft infection.J Vasc Surg. 2020 Dec;72(6):2174-2185.e2. doi: 10.1016/j.jvs.2020.05.065. Epub 2020 Jul 6. J Vasc Surg. 2020. PMID: 32645420
-
Hyperaccumulation of (18)F-FDG in order to differentiate solid pseudopapillary tumors from adenocarcinomas and from neuroendocrine pancreatic tumors and review of the literature.Hell J Nucl Med. 2013 May-Aug;16(2):97-102. doi: 10.1967/s002449910084. Epub 2013 May 20. Hell J Nucl Med. 2013. PMID: 23687644 Review.
Cited by
-
Knowledge mapping of macrophage and its role in aneurysm from 1999 to 2022: A bibliometric analysis.Heliyon. 2024 Jul 30;10(15):e35212. doi: 10.1016/j.heliyon.2024.e35212. eCollection 2024 Aug 15. Heliyon. 2024. PMID: 39166074 Free PMC article.
References
-
- Casali M, Lauri C, Altini C, Bertagna F, Cassarino G, Cistaro A, Erba AP, Ferrari C, Mainolfi CG, Palucci A, Prandini N, Baldari S, Bartoli F, Bartolomei M, D'Antonio A, Dondi F, Gandolfo P, Giordano A, Laudicella R, Massollo M, Nieri A, Piccardo A, Vendramin L, Muratore F, Lavelli V, Albano D, Burroni L, Cuocolo A, Evangelista L, Lazzeri E, Quartuccio N, Rossi B, Rubini G, Sollini M, Versari A, Signore A. State of the art of (18)F-FDG PET/CT application in inflammation and infection: a guide for image acquisition and interpretation. Clin Transl Imaging. 2021;9:299–339. - PMC - PubMed
-
- Arnon-Sheleg E, Keidar Z. Vascular Graft Infection Imaging. Semin Nucl Med. 2023;53:70–77. - PubMed
-
- Bowles H, Ambrosioni J, Mestres G, Hernández-Meneses M, Sánchez N, Llopis J, Yugueros X, Almela M, Moreno A, Riambau V, Fuster D, Miró JM Hospital Clinic Endocarditis Study Group. Diagnostic yield of (18)F-FDG PET/CT in suspected diagnosis of vascular graft infection: A prospective cohort study. J Nucl Cardiol. 2020;27:294–302. - PubMed
-
- Chrapko BE, Chrapko M, Nocuń A, Zubilewicz T, Stefaniak B, Mitura J, Wolski A, Terelecki P. Patterns of vascular graft infection in 18F-FDG PET/CT. Nucl Med Rev Cent East Eur. 2020;23:63–70. - PubMed
-
- Schaefers JF, Donas KP, Panuccio G, Kasprzak B, Heine B, Torsello GB, Osada N, Usai MV. Outcomes of Surgical Explantation of Infected Aortic Grafts After Endovascular and Open Abdominal Aneurysm Repair. Eur J Vasc Endovasc Surg. 2019;57:130–136. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
