

A Case of an Elderly Woman Who Developed Corneal Perforation in the Clinical Course of Myeloperoxidase Positive Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
- PMID: 37662600
- PMCID: PMC10474959
- DOI: 10.1155/2023/4246075
A Case of an Elderly Woman Who Developed Corneal Perforation in the Clinical Course of Myeloperoxidase Positive Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
Abstract
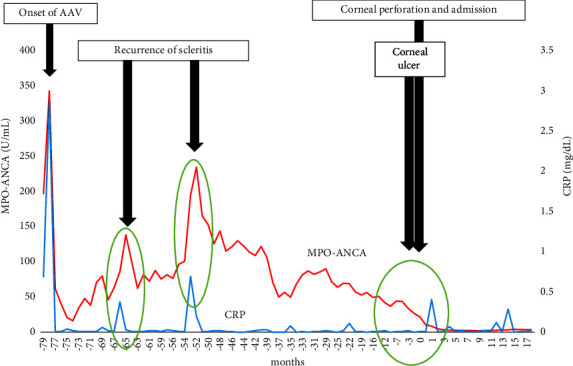
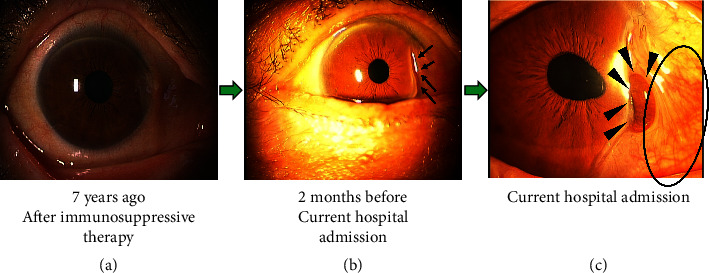
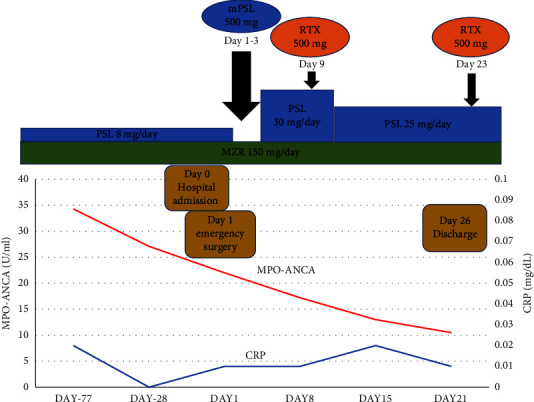
Antineutrophil cytoplasmic antibody- (ANCA-) associated vasculitis (AAV) is a systemic vasculitis characterized by ANCA positivity and categorized into three main types: microscopic polyangiitis, granulomatosis with polyangiitis, and eosinophilic granulomatous with polyangiitis. Although AAV leads to systemic organ injury, such as of the lungs, kidneys, nerves, and skin, patients with AAV sometimes develop ocular lesions. Here, we report the case of an elderly woman who had been treated for AAV for seven years. She developed scleritis and relapsed twice, with elevation of serum disease markers such as ANCA titer and C-reactive protein. After the decline of these markers due to treatment with additional medication, her scleritis relapsed again and caused a corneal ulcer, which resulted in perforation without obvious marker elevation. She did not present with any symptoms of organ injury, except for ocular lesions. She was treated with surgery, followed by methylprednisolone and rituximab therapy. Subsequently, her ocular lesions and symptoms improved, and she did not relapse. AAV can cause various ocular manifestations. Although C-reactive protein and ANCA titers are useful markers of disease activity and the relapse of AAV complications, including ocular lesions, these markers do not always increase at the time of worsening ocular lesions. Therefore, it is important for clinicians treating patients with AAV to pay careful attention to serum data and physical findings, including the eyes.
Copyright © 2023 Shuhei Kobayashi et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Development of eosinophilic granulomatosis with polyangiitis during the clinical course of microscopic polyangiitis: A case report.Medicine (Baltimore). 2022 Nov 4;101(44):e31401. doi: 10.1097/MD.0000000000031401. Medicine (Baltimore). 2022. PMID: 36343053 Free PMC article.
-
Cutaneous manifestations of antineutrophil cytoplasmic antibody-associated vasculitis (AAV): a concise review with emphasis on clinical and histopathologic correlation.Int J Dermatol. 2022 Dec;61(12):1442-1451. doi: 10.1111/ijd.16247. Epub 2022 May 22. Int J Dermatol. 2022. PMID: 35599359 Review.
-
A Case of Pleuritis Associated With Antineutrophil Cytoplasmic Antibody (ANCA)-Associated Vasculitis Diagnosed Through Medical Thoracoscopy.Cureus. 2024 Sep 21;16(9):e69827. doi: 10.7759/cureus.69827. eCollection 2024 Sep. Cureus. 2024. PMID: 39435223 Free PMC article.
-
Clinical characteristics, the diagnostic criteria and management recommendation of otitis media with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (OMAAV) proposed by Japan Otological Society.Auris Nasus Larynx. 2021 Feb;48(1):2-14. doi: 10.1016/j.anl.2020.07.004. Epub 2020 Aug 5. Auris Nasus Larynx. 2021. PMID: 32768313 Review.
-
Diagnostic algorithm for antineutrophil cytoplasmic antibody-associated systemic vasculitis.Ter Arkh. 2018 May 11;90(5):13-22. doi: 10.26442/terarkh201890513-22. Ter Arkh. 2018. PMID: 30701885
Cited by
-
Isolated ANCA-associated scleritis successfully treated with systemic rituximab; a case report and review of literature.BMC Ophthalmol. 2025 Apr 7;25(1):176. doi: 10.1186/s12886-025-04027-6. BMC Ophthalmol. 2025. PMID: 40197146 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
