

Management Paradigm of Central Nervous System Metastases in NSCLC: An Australian Perspective
- PMID: 37663675
- PMCID: PMC10472312
- DOI: 10.1016/j.jtocrr.2023.100553
Management Paradigm of Central Nervous System Metastases in NSCLC: An Australian Perspective
Abstract
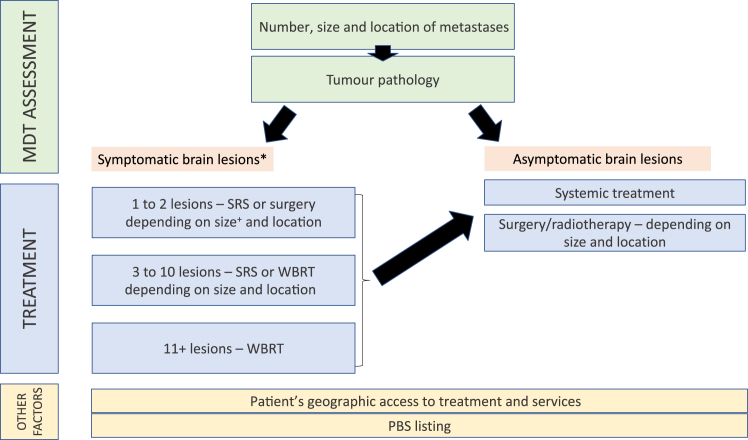
Life-prolonging central nervous system active systemic therapies for metastatic NSCLC have increased the complexity of managing brain metastases (BMs). Australian medical oncologists, radiation oncologists, and neurosurgeons discussed the evidence guiding the diverse clinical approaches to the management of BM in NSCLC. The Australian context is broadly applicable to other jurisdictions; therefore, we have documented these discussions as principles with broader applications. Patient management was stratified according to clinical and radiologic factors under two broad classifications of newly diagnosed BMs: symptomatic and asymptomatic. Other important considerations include the number and location of metastases, tumor histotypes, molecular subtype, and treatment purpose. Careful consideration of the pace and burden of symptoms, risk of worsening neurologic function at a short interval, and extracranial disease burden should determine whether central nervous system active systemic therapies are used alone or in combination with local therapies (surgery with or without radiation therapy). Most clinical trial evidence currently focuses on historical treatment options or a single treatment modality rather than the optimal sequencing of multiple modern therapies; therefore, an individualized approach is key in a rapidly changing therapeutic landscape.
Keywords: Brain metastases; Molecular targeted therapy; Neurosurgical procedures; Non–small cell lung cancer; Radiotherapy.
© 2023 by the International Association for the Study of Lung Cancer.
Figures
References
-
- Wolf A., Kvint S., Chachoua A., et al. Toward the complete control of brain metastases using surveillance screening and stereotactic radiosurgery. J Neurol Surg. 2018;128:23–31. - PubMed
-
- Vogelbaum M.A., Brown P.D., Messersmith H., et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J Clin Oncol. 2022;40:492–516. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
