

Phase 3 CLEAR study in patients with advanced renal cell carcinoma: outcomes in subgroups for the lenvatinib-plus-pembrolizumab and sunitinib arms
- PMID: 37664025
- PMCID: PMC10471185
- DOI: 10.3389/fonc.2023.1223282
Phase 3 CLEAR study in patients with advanced renal cell carcinoma: outcomes in subgroups for the lenvatinib-plus-pembrolizumab and sunitinib arms
Erratum in
-
Corrigendum: Phase 3 CLEAR study in patients with advanced renal cell carcinoma: outcomes in subgroups for the lenvatinib-plus-pembrolizumab and sunitinib arms.Front Oncol. 2024 Mar 1;13:1343027. doi: 10.3389/fonc.2023.1343027. eCollection 2023. Front Oncol. 2024. PMID: 38495081 Free PMC article.
Abstract
Introduction: The phase 3 CLEAR study demonstrated that lenvatinib plus pembrolizumab significantly improved efficacy versus sunitinib as first-line treatment for patients with advanced renal cell carcinoma (RCC). Prognostic features including presence and/or site of baseline metastases, prior nephrectomy, and sarcomatoid features have been associated with disease and treatment success. This subsequent analysis explores outcomes in patients with or without specific prognostic features.
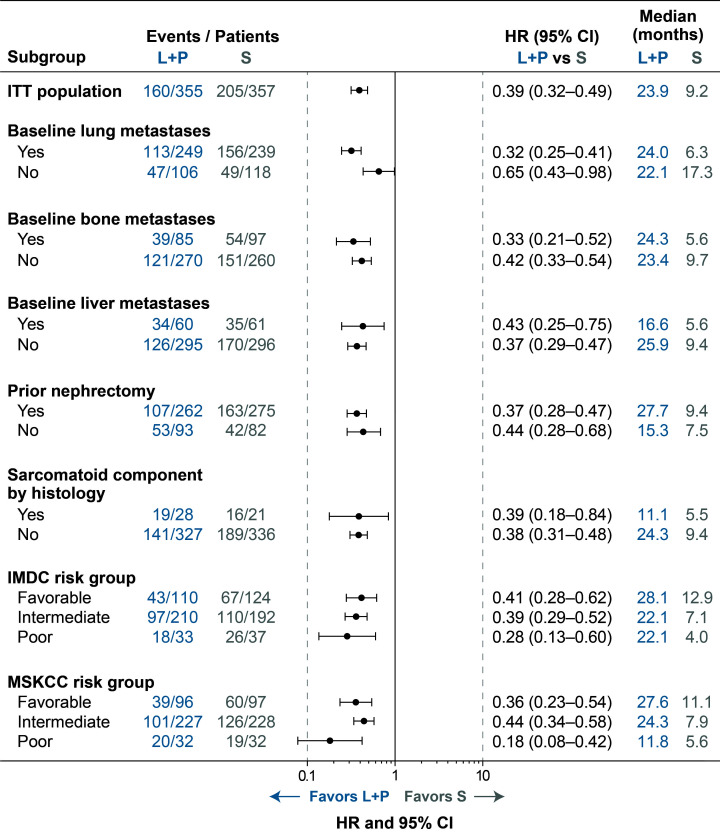
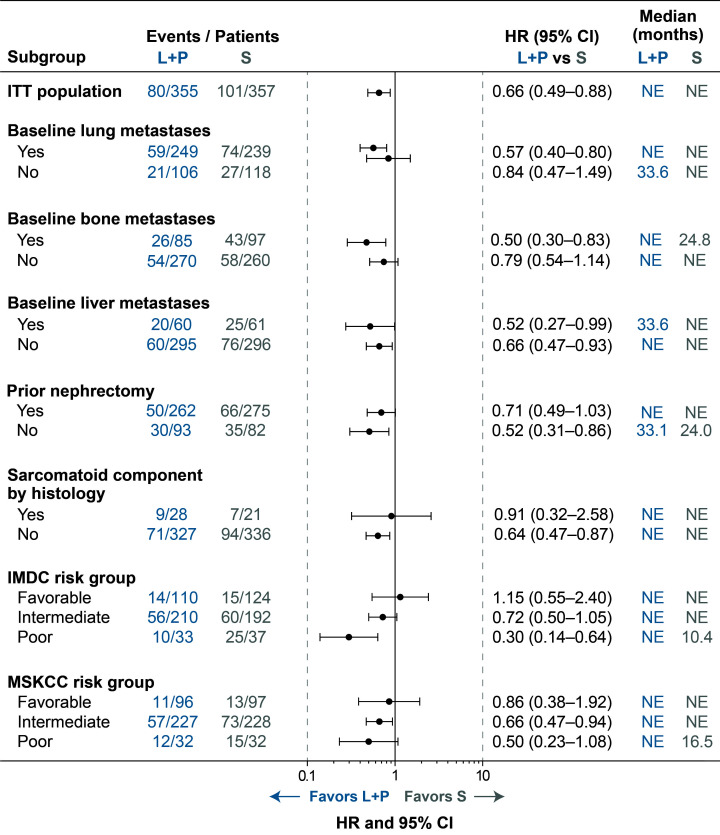
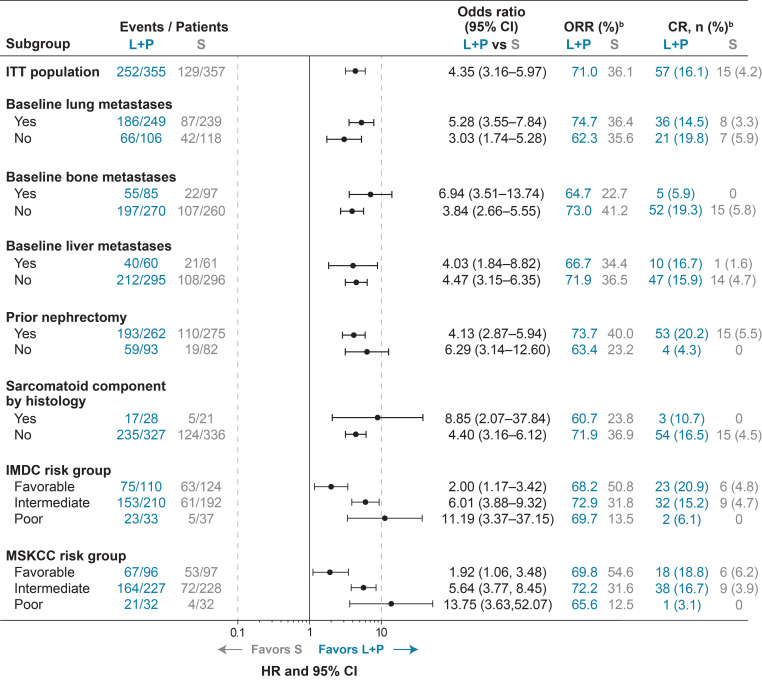
Methods: In CLEAR, patients with clear cell RCC were randomly assigned (1:1:1) to receive either lenvatinib (20 mg/day) plus pembrolizumab (200 mg every 3 weeks), lenvatinib (18 mg/day) plus everolimus (5 mg/day), or sunitinib alone (50 mg/day, 4 weeks on, 2 weeks off). In this report, progression-free survival (PFS), overall survival (OS), and objective response rate (ORR) were all assessed in the lenvatinib-plus-pembrolizumab and the sunitinib arms, based on baseline features: lung metastases, bone metastases, liver metastases, prior nephrectomy, and sarcomatoid histology.
Results: In all the assessed subgroups, median PFS was longer with lenvatinib-plus-pembrolizumab than with sunitinib treatment, notably among patients with baseline bone metastases (HR 0.33, 95% CI 0.21-0.52) and patients with sarcomatoid features (HR 0.39, 95% CI 0.18-0.84). Median OS favored lenvatinib plus pembrolizumab over sunitinib irrespective of metastatic lesions at baseline, prior nephrectomy, and sarcomatoid features. Of interest, among patients with baseline bone metastases the HR for survival was 0.50 (95% CI 0.30-0.83) and among patients with sarcomatoid features the HR for survival was 0.91 (95% CI 0.32-2.58); though for many groups, median OS was not reached. ORR also favored lenvatinib plus pembrolizumab over sunitinib across all subgroups; similarly, complete responses also followed this pattern.
Conclusion: Efficacy outcomes improved following treatment with lenvatinib-plus-pembrolizumab versus sunitinib in patients with RCC-irrespective of the presence or absence of baseline lung metastases, baseline bone metastases, baseline liver metastases, prior nephrectomy, or sarcomatoid features. These findings corroborate those of the primary CLEAR study analysis in the overall population and support lenvatinib plus pembrolizumab as a standard of care in 1L treatment for patients with advanced RCC.
Clinical trial registration: ClinicalTrials.gov, identifier NCT02811861.
Keywords: bone metastases; lenvatinib; liver metastases; lung metastases; pembrolizumab; renal cell carcinoma; sarcomatoid histology; sunitinib.
Copyright © 2023 Grünwald, Powles, Eto, Kopyltsov, Rha, Porta, Motzer, Hutson, Méndez-Vidal, Hong, Winquist, Goh, Maroto, Buchler, Takagi, Burgents, Perini, He, Okpara, McKenzie and Choueiri.
Conflict of interest statement
VG: Invited Speaker: AstraZeneca, Astellas, BMS, EISAI, Ipsen, Janssen-Cilag, Merck, MSD, Pfizer, ONO Pharmaceutical, Novartis/AAA; Advisory Board: Apogepha, BMS, EISAI, EUSA Pharm, Cureteq, Debiopharm, Gilead, Janssen-Cilag, Merck, MSD, Pfizer, Novartis, Oncorena, PCI Biotech; Stocks/Shares: AstraZeneca, BMS, MSD, SeaGen; Steering Committee Member: BMS, EISAI, Ipsen, Novartis, PharmaMar; Travel support: AstraZeneca, Ipsen, Merck, Janssen, Pfizer. Non-Financial Interests: Membership: ASCO, ESMO, German medical Oncology and Hematology Society; Advisory role: German Cancer Society; Leadership role: Working Group medical oncology (AIO). TP: reports research funding from Astellas Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, Exelixis, Ipsen, Johnson & Johnson, Merck, Merck Serono, MSD, Novartis, Pfizer, Roche, and Seattle Genetics; consulting fees from Astellas Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, Exelixis, Incyte, Ipsen, Johnson & Johnson, Merck, Merck Serono, MSD, Novartis, Pfizer, Roche, and Seattle Genetics; support for attending meetings or travel from Astra Zeneca, Ipsen, MSD, Pfizer, and Roche. ME: reports research funding from Kissei, Sanofi, Astellas, ONO, Takeda, and Bayer; and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from MSD, ONO, Chugai, Novartis, Pfizer, Bristol Myers Squibb, Takeda, Janssen, and Merck. SYR: reports grants or contracts from Amgen, Merck, Bristol Myers Squibb, MSD, Lilly, Daiichi Sankyo, Beigene, Eisai, and AstraZeneca; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Amgen, Lilly, Bristol Myers Squibb, MSD, and Eisai; and participation on a data safety monitoring board or advisory board from Amgen, MSD, Bristol Myers Squibb, Merck, Indivumed, Beigene, Eisai, and Daiichi Sankyo. CP: reports consulting fees from Angelini Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, Ipsen, and MSD; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Angelini Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, General Electric, Ipsen, and MSD; and participation on a data safety monitoring board or advisory board for Bristol Myers Squibb, Eisai, MSD, the European Society of Medical Oncology, and the Italian Association for Medical Oncology. RM: reports research funding, paid to their institution from Bristol Myers Squibb, Eisai, Exelixis, Genentech/Roche, Merck, Pfizer, and Aveo Pharmaceuticals and consulting fees from AstraZeneca, Aveo Pharmaceuticals, Eisai, EMD Serono, Exelixis, Genentech/Roche, Incyte, Lilly, Merck, Novartis, Pfizer, and Takeda. TEH: reports grants or contracts, paid to their institution, from Bristol Myers Squibb, Eisai, Exelixis, Johnson & Johnson, and Pfizer; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Astellas Pharma, Bristol Myers Squibb, Eisai, Exelixis, Johnson & Johnson, and Pfizer; and participation on a data safety monitoring board or advisory board for Astellas Pharma, Bayer/Onyx, Bristol Myers Squibb, Exelixis, Johnson & Johnson, Novartis, and Pfizer. MJM-V: reports consulting fees from Astellas Pharma, Bristol Myers Squibb, EUSA Pharma, Ipsen, Eisai, Janssen-Cilag, Novartis, Pfizer, Roche, and Sanofi; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Astellas Pharma, Bristol Myers Squibb, Ipsen, EUSA Pharma, Janssen-Cilag, Pfizer, and Roche; and support for attending meetings or travel from Astellas Pharma, Bristol Myers Squibb, Ipsen, Janssen-Cilag, Pfizer, and Roche. EW: reports research support, paid to their institution from Ayala Pharmaceuticals, Eisai, Merck, Pfizer, and Roche/Genentech; honoraria from Amgen, Bayer, Eisai, Merck, and Roche. JCG: reports consulting fees for an advisory board meeting from MSD Australia, Bristol Myers Squibb, and GlaxoSmithKline; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Janssen–Cilag, Ipsen, MSD Australia, and AstraZeneca Australia; and support for attending meetings or travel from AstraZeneca Australia, GlaxoSmithKline, and Pfizer. PM: reports research support, paid to their institution from Roche. TB: reports institutional research support from AstraZeneca, Roche, Bristol Myers Squibb, Exelixis, Merck, and Novartis; consulting fees from Bristol Myers Squibb, Astellas, Janssen, and Sanofi/Aventis; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Ipsen, Bristol Myers Squibb, Servier, and Pfizer; and institutional receipt of equipment, materials, drugs, medical writing, gifts, or other services from Bristol Myers Squibb, AstraZeneca, Roche, and Servier. TT: reports honoraria from Bristol Myers Squibb, Eisai, and Ono Pharmaceutical. JEB: employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. RP: employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. CH: employee of Eisai Inc. CO: employee of Eisai Ltd. JM: employee of Eisai Inc. TKC: reports institutional and/or personal, paid and/or unpaid support for research, advisory boards, consultancy, and honoraria from: Alkermes, AstraZeneca, Aravive, Aveo, Bayer, Bristol Myers Squibb, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, Gilead, IQVA, Infinity, Ipsen, Jansen, Kanaph, Lilly, Merck, Nikang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Scholar Rock, Surface Oncology, Takeda, Tempest, Up-To-Date, CME events Peerview, OncLive, MJH and others, outside the submitted work. Institutional patents filed on molecular alterations and immunotherapy response/toxicity, and ctDNA. Equity: Tempest, Pionyr, Osel, Precede Bio, CureResponse. Committees: NCCN, GU Steering Committee, ASCO/ESMO, ACCRU, KidneyCan. Medical writing and editorial assistance support may have been funded by Communications companies in part. No speaker’s bureau. Mentored several non-US citizens on research projects with potential funding in part from non-US sources/Foreign Components. The institution Dana-Farber Cancer Institute may have received additional independent funding of drug companies or/and royalties potentially involved in research around the subject matter. TKC is supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE 2P50CA101942-16 and Program 5P30CA006516-56, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, Pan Mass Challenge, Hinda and Arthur Marcus Fund and Loker Pinard Funds for Kidney Cancer Research at DFCI. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical