

NephroCheck at 10: addressing unmet needs in AKI diagnosis and risk stratification
- PMID: 37664563
- PMCID: PMC10468756
- DOI: 10.1093/ckj/sfad146
NephroCheck at 10: addressing unmet needs in AKI diagnosis and risk stratification
Abstract
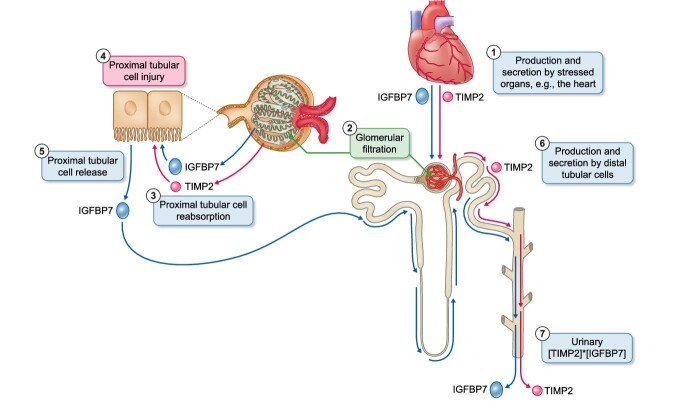
Despite its name, the current diagnosis of acute kidney injury (AKI) still depends on markers of decreased kidney function and not on markers of injury. This results in a delayed diagnosis: AKI is diagnosed based on serum creatinine criteria only when the severity of injury is enough to decrease glomerular filtration rate. Moreover, by the time AKI is diagnosed, the insult may have already ceased, and even appropriate therapy targeted at the specific insult and its associated pathogenic pathways may no longer be effective. Biomarkers of injury are needed that allow the diagnosis of AKI based on injury criteria. At least three commercially available immunoassays assessing urinary or plasma neutrophil gelatinase-associated lipocalin and urinary tissue inhibitor of metalloproteinases-2 × insulin-like growth factor-binding protein-7 ([TIMP2]*[IGFBP7]) (NephroCheck®) have generated promising data regarding prediction and early diagnosis of AKI, although their relative performance may depend on clinical context. Recently, a urinary peptidomics classifier (PeptAKI) was reported to predict AKI better than current biomarkers. Focusing on [TIMP2]*[IGFBP7], the cellular origin of urinary TIMP2 and IGFBP7 remains unclear, especially under the most common predisposing condition for AKI, i.e. chronic kidney disease. We now discuss novel data on the kidney cell expression of TIMP2 and IGFBP7 and its clinical implications.
Keywords: IGFBP7; NGAL; NephroCheck; TIMP2; acute kidney injury; biomarkers; chronic kidney disease; urinary proteomics.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
A.O. has received grants from Sanofi and consultancy or speaker fees or travel support from Adviccene, Alexion, Astellas, AstraZeneca, Amicus, Amgen, Boehringer Ingelheim, Fresenius Medical Care, GSK, Bayer, Sanofi-Genzyme, Menarini, Mundipharma, Kyowa Kirin, Lilly, Freeline, Idorsia, Chiesi, Otsuka, Novo-Nordisk, Sysmex and Vifor Fresenius Medical Care Renal Pharma, and is Director of the Catedra Mundipharma-UAM of diabetic kidney disease and the Catedra AstraZeneca-UAM of chronic kidney disease and electrolytes. He has stock in Telara Farma and is a previous CKJ Editor-in-Chief.
Figures
References
-
- Zarbock A, Küllmar M, Ostermann Met al. Prevention of cardiac surgery-associated acute kidney injury by implementing the KDIGO guidelines in high-risk patients identified by biomarkers: the PrevAKI-multicenter randomized controlled trial. Anesth Analg 2021;133:292–302. 10.1213/ANE.0000000000005458 - DOI - PubMed
-
- El-Khoury JM, Hoenig MP, Jones GRDet al. AACC guidance document on laboratory investigation of acute kidney injury. J Appl Lab Med 2021;6:1316–37. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
