

Long-term effect of acute ischemic injury on the kidney underwent clamped partial nephrectomy
- PMID: 37664597
- PMCID: PMC10474450
- DOI: 10.1016/j.isci.2023.107610
Long-term effect of acute ischemic injury on the kidney underwent clamped partial nephrectomy
Abstract
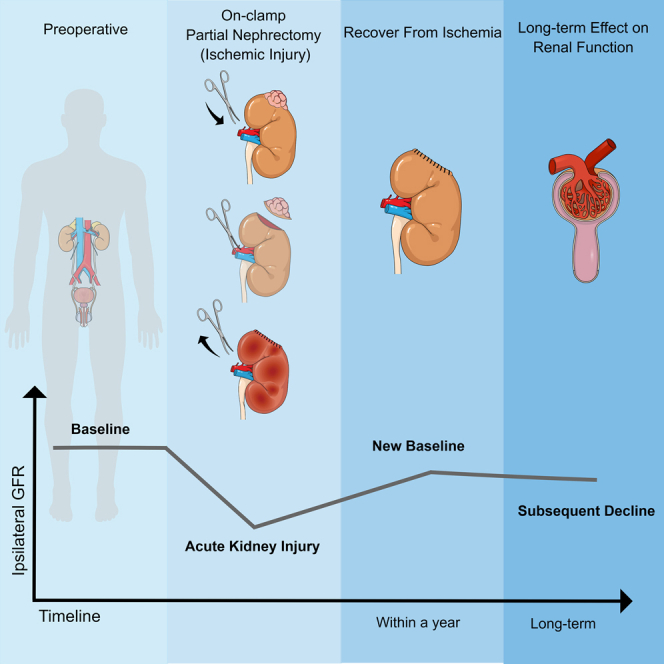
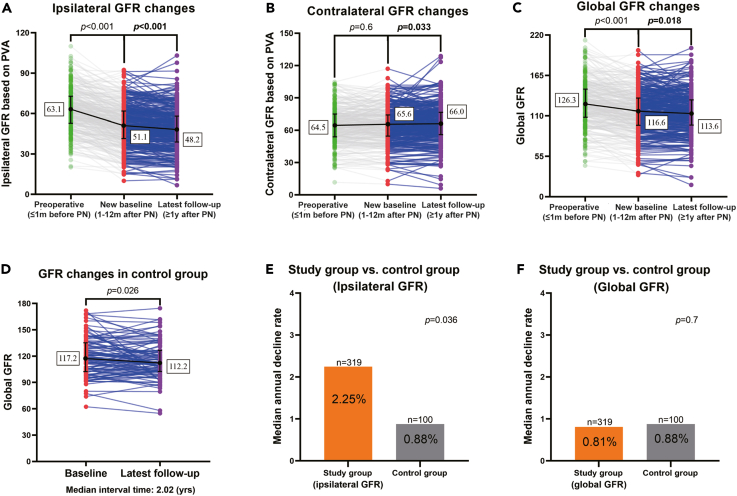
GFR reaches a new baseline, primarily correlating with nephron-mass preservation, 1-12 months after partial nephrectomy (PN). However, does the ipsilateral GFR experience subsequent decline, and does acute ischemic injury has long-term effect on the operated kidney? 319 patients with two kidneys and unilateral clamped PN were analyzed. All had preoperative, new-baseline, and latest follow-up imaging/serum creatinine levels. Annual ipsilateral GFR decline rate (AIGDR) was defined as new-baseline GFR minus latest follow-up GFR normalized by new-baseline GFR, per year. Spectrum score was used to reflect the degree of acute ischemic injury in the operated kidney. 100 subjects searching for health screening served as controls. Predictive factors for AIGDR were assessed. The median AIGDR was 2.25%, significantly higher than controls (0.88%, p = 0.036). With some contralateral hypertrophy, the global annual GFR decline was similar to that of controls (0.81% vs. 0.88%, p = 0.7). Spectrum score correlated significantly with AIGDR (p = 0.037). These results support that acute ischemic injury has long-term effect on the operated kidney.
Keywords: Endocrinology; Medical endocrinology; Pathophysiology; Public health.
© 2023 The Authors.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Longitudinal changes in renal parenchymal volume and function status after partial nephrectomy: a retrospective cohort study.Int J Surg. 2024 Feb 1;110(2):984-991. doi: 10.1097/JS9.0000000000000938. Int J Surg. 2024. PMID: 38000077 Free PMC article.
-
Acute Ipsilateral Renal Dysfunction after Partial Nephrectomy in Patients with a Contralateral Kidney: Spectrum Score to Unmask Ischemic Injury.Eur Urol. 2016 Oct;70(4):692-698. doi: 10.1016/j.eururo.2016.04.015. Epub 2016 Apr 28. Eur Urol. 2016. PMID: 27131953
-
Ischemia and Functional Recovery from Partial Nephrectomy: Refined Perspectives.Eur Urol Focus. 2018 Jul;4(4):572-578. doi: 10.1016/j.euf.2017.02.001. Epub 2017 Mar 3. Eur Urol Focus. 2018. PMID: 28753855
-
Decline in renal function after partial nephrectomy: etiology and prevention.J Urol. 2015 Jun;193(6):1889-98. doi: 10.1016/j.juro.2015.01.093. Epub 2015 Jan 29. J Urol. 2015. PMID: 25637858 Review.
-
Renal Preservation and Partial Nephrectomy: Patient and Surgical Factors.Eur Urol Focus. 2016 Dec 15;2(6):589-600. doi: 10.1016/j.euf.2017.02.012. Epub 2017 Mar 16. Eur Urol Focus. 2016. PMID: 28723490 Review.
Cited by
-
Ultrasound-guided renal artery balloon catheter occluded hybrid partial nephrectomy (UBo-HPN) with branch renal artery occlusion: a single arm trial.World J Urol. 2024 Oct 9;42(1):570. doi: 10.1007/s00345-024-05263-z. World J Urol. 2024. PMID: 39382799 Free PMC article.
References
-
- Cerrato C., Patel D., Autorino R., Simone G., Yang B., Uzzo R., Porpiglia F., Capitanio U., Porter J., Beksac A.T., et al. Partial or radical nephrectomy for complex renal mass: a comparative analysis of oncological outcomes and complications from the rosula (robotic surgery for large renal mass) collaborative group. World J. Urol. 2023;41:747–755. doi: 10.1007/s00345-023-04279-1. - DOI - PubMed
-
- Simone G., Gill I.S., Mottrie A., Kutikov A., Patard J.J., Alcaraz A., Rogers C.G. Indications, techniques, outcomes, and limitations for minimally ischemic and off-clamp partial nephrectomy: a systematic review of the literature. Eur. Urol. 2015;68:632–640. doi: 10.1016/j.eururo.2015.04.020. - DOI - PubMed
LinkOut - more resources
Full Text Sources
