

Classification and Predictors of Right Ventricular Functional Recovery in Pulmonary Arterial Hypertension
- PMID: 37664964
- PMCID: PMC10592283
- DOI: 10.1161/CIRCHEARTFAILURE.123.010555
Classification and Predictors of Right Ventricular Functional Recovery in Pulmonary Arterial Hypertension
Abstract
Background: Normative changes in right ventricular (RV) structure and function have not been characterized in the context of treatment-associated functional recovery (RV functional recovery [RVFnRec]). The aim of this study is to assess the clinical relevance of a proposed RVFnRec definition.
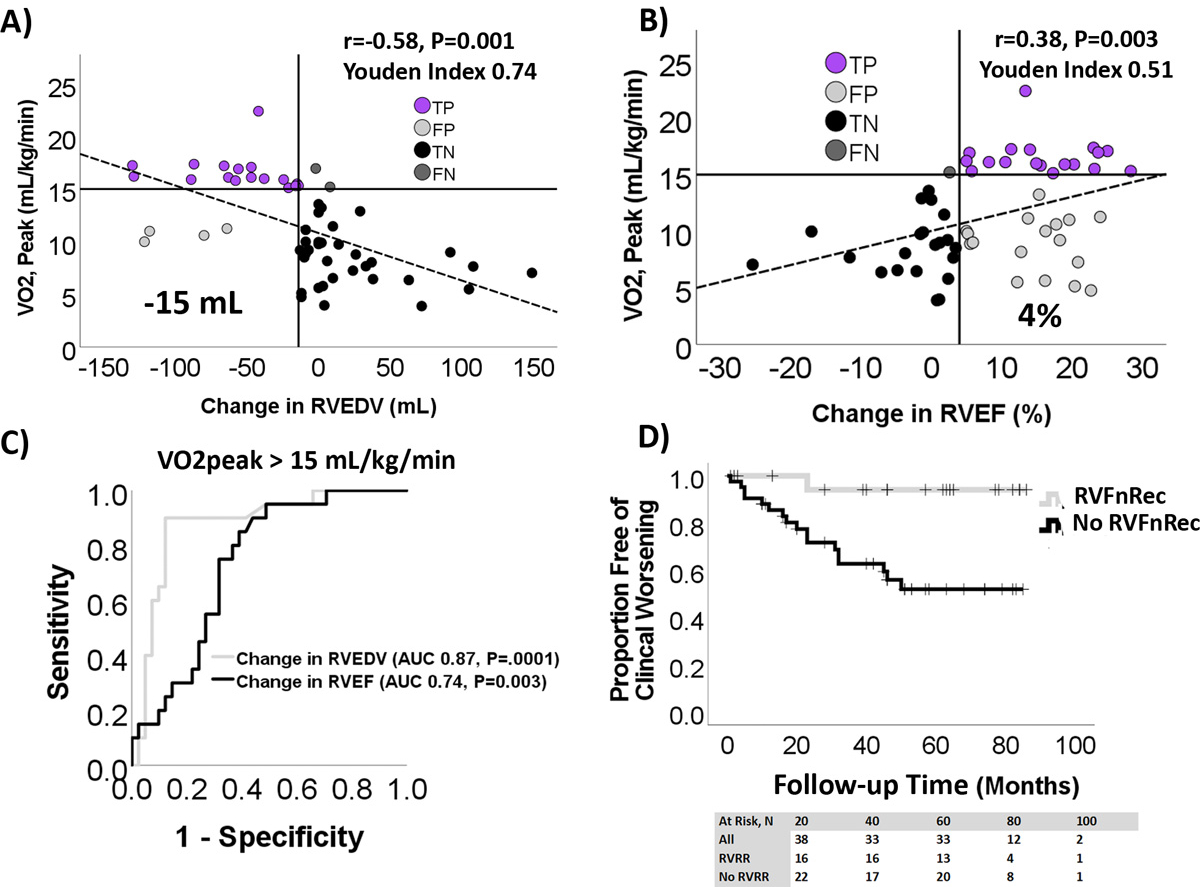
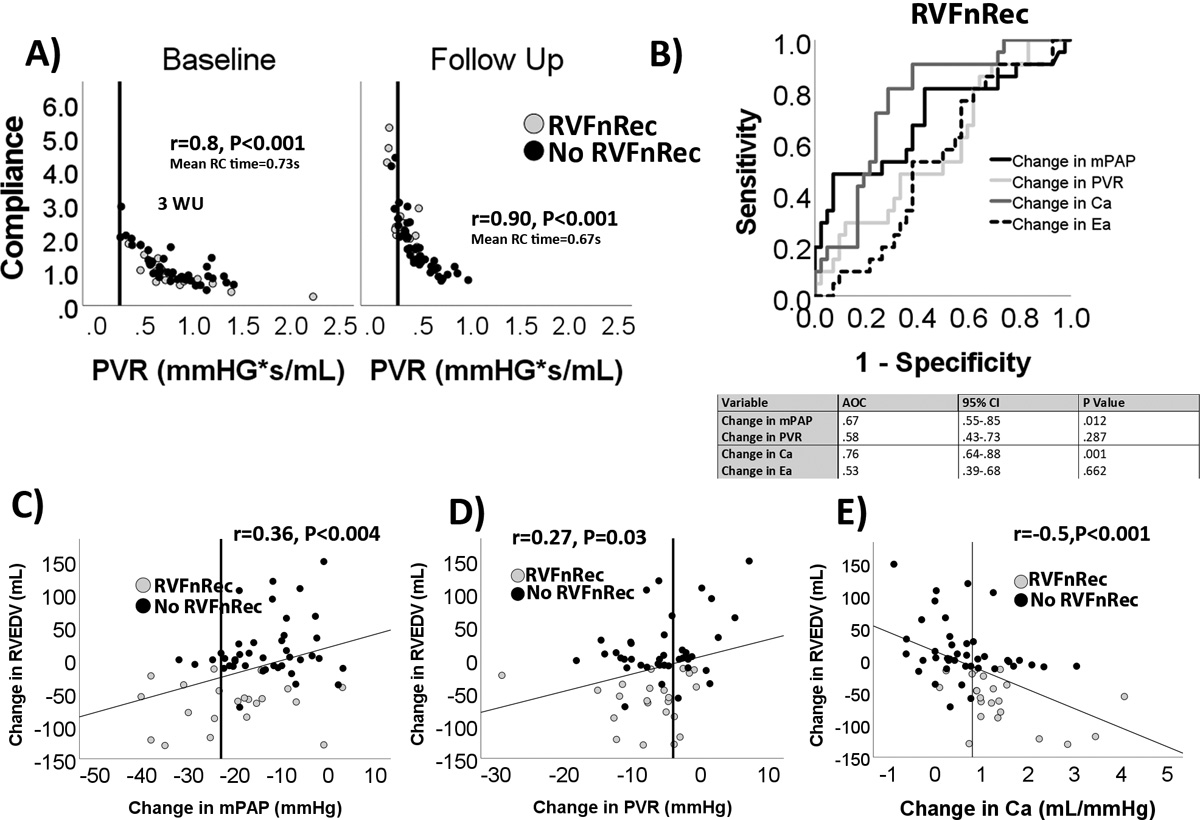
Methods: We evaluated 63 incident patients with pulmonary arterial hypertension by right heart catheterization and cardiac magnetic resonance imaging at diagnosis and cardiac magnetic resonance imaging and invasive cardiopulmonary exercise testing following treatment (≈11 months). Sex, age, ethnicity matched healthy control subjects (n=62) with 1-time cardiac magnetic resonance imaging and noninvasive cardiopulmonary exercise testing were recruited from the PVDOMICS (Redefining Pulmonary Hypertension through Pulmonary Vascular Disease Phenomics) project. We examined therapeutic cardiac magnetic resonance imaging changes relative to the evidence-based peak oxygen consumption (VO2peak)>15 mL/(kg·min) to define RVFnRec by receiver operating curve analysis. Afterload was measured as mean pulmonary artery pressure, resistance, compliance, and elastance.
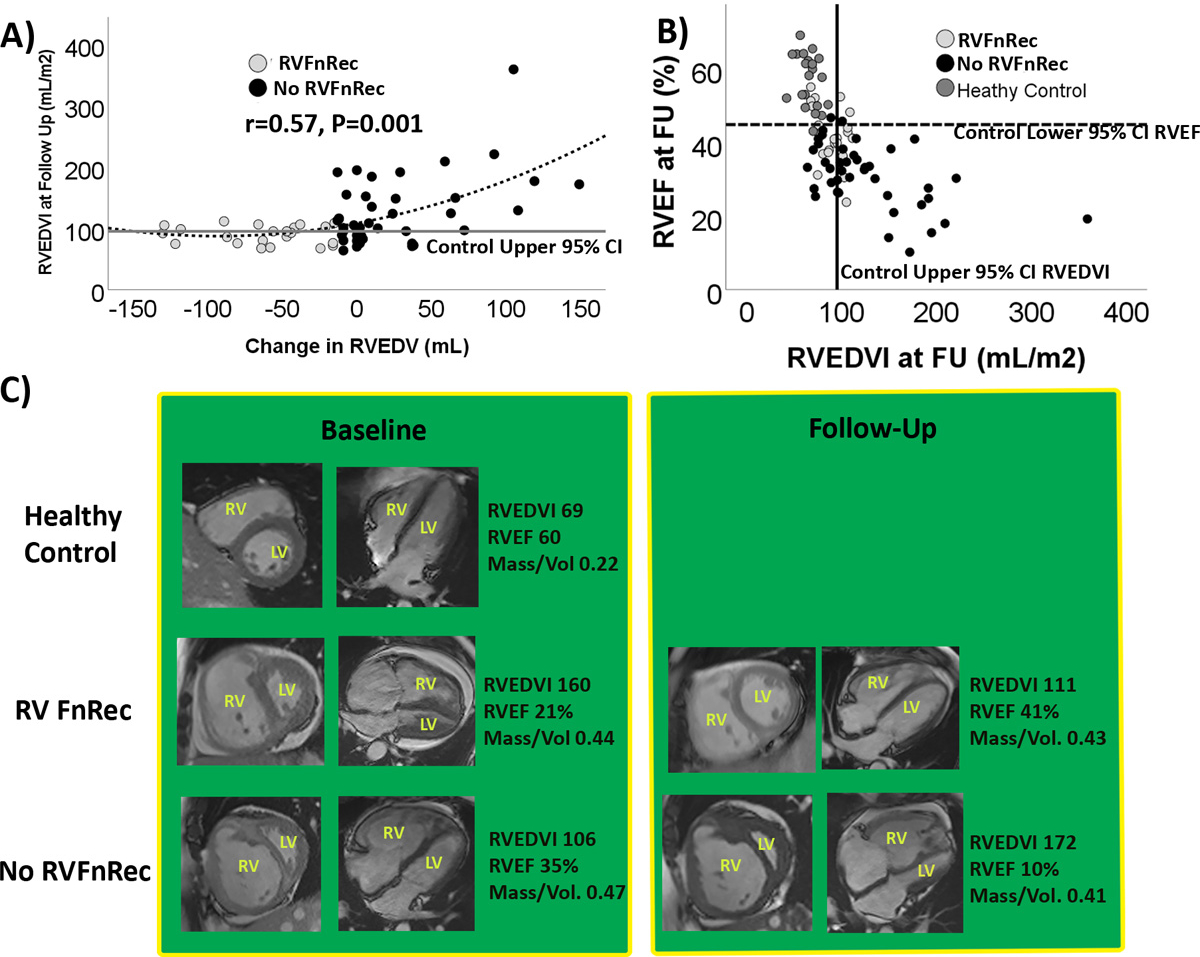
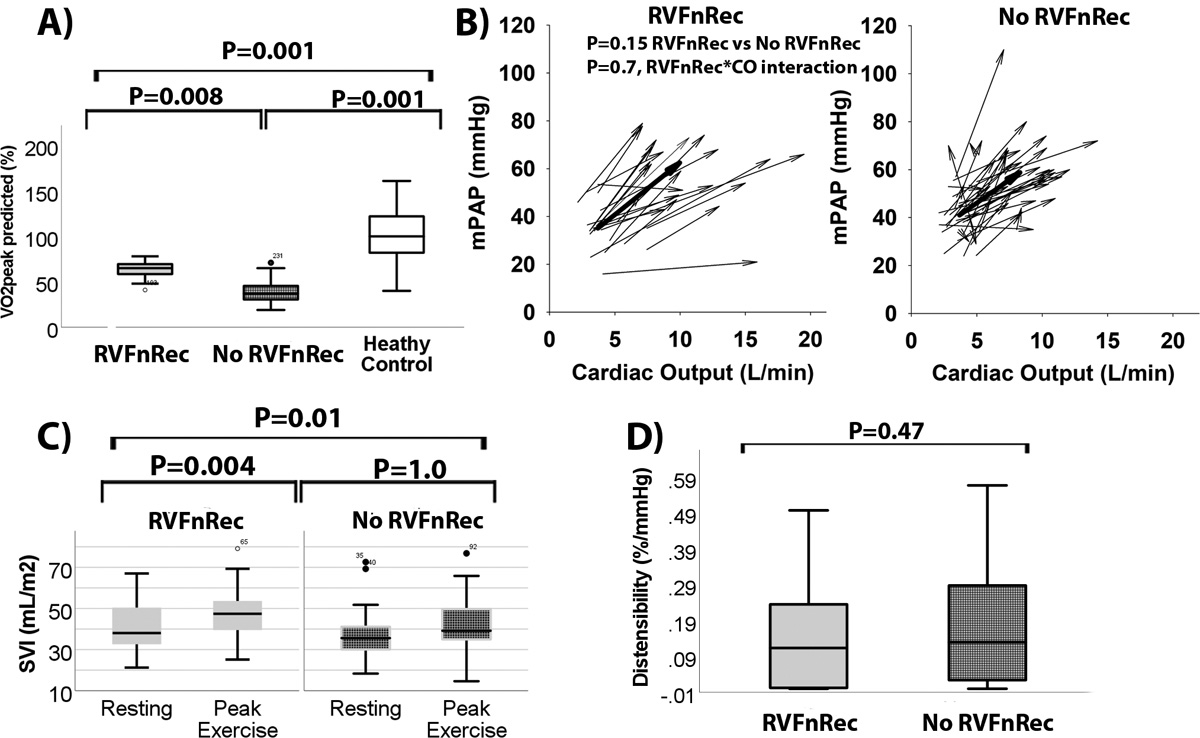
Results: A drop in RV end-diastolic volume of -15 mL best defined RVFnRec (area under the curve, 0.87; P=0.0001) and neared upper 95% CI RV end-diastolic volume of controls. This cutoff was met by 22 out of 63 (35%) patients which was reinforced by freedom from clinical worsening, RVFnRec 1 out of 21 (5%) versus no RVFnRec 17 out of 42, 40% (log-rank P=0.006). A therapy-associated increase of 0.8 mL/mm Hg in compliance had the best predictive value of RVFnRec (area under the curve, 0.76; [95% CI, 0.64-0.88]; P=0.001). RVFnRec patients had greater increases in stroke volume, and cardiac output at exercise.
Conclusions: RVFnRec defined by RV end-diastolic volume therapeutic decrease of -15 mL predicts exercise capacity, freedom from clinical worsening, and nears normalization. A therapeutic improvement of compliance is superior to other measures of afterload in predicting RVFnRec. RVFnRec is also associated with increased RV output reserve at exercise.
Keywords: catheterization; exercise; hypertension, pulmonary; magnetic resonance imaging; oxygen consumption.
Conflict of interest statement
Figures
Update of
-
Classification and Predictors of Right Ventricular Functional Recovery in Pulmonary Arterial Hypertension.medRxiv [Preprint]. 2023 Feb 16:2023.02.15.23285974. doi: 10.1101/2023.02.15.23285974. medRxiv. 2023. Update in: Circ Heart Fail. 2023 Oct;16(10):e010555. doi: 10.1161/CIRCHEARTFAILURE.123.010555. PMID: 36824981 Free PMC article. Updated. Preprint.
References
-
- Leopold JA, Kawut SM, Aldred MA, Archer SL, Benza RL, Bristow MR, Brittain EL, Chesler N, DeMan FS, Erzurum SC, et al. Diagnosis and Treatment of Right Heart Failure in Pulmonary Vascular Diseases: A National Heart, Lung, and Blood Institute Workshop. Circ Heart Fail. 2021;14:e000069. doi: 10.1161/CIRCHEARTFAILURE.120.007975 - DOI - PMC - PubMed
-
- Lahm T, Douglas IS, Archer SL, Bogaard HJ, Chesler NC, Haddad F, Hemnes AR, Kawut SM, Kline JA, Kolb TM, et al. Assessment of Right Ventricular Function in the Research Setting: Knowledge Gaps and Pathways Forward. An Official American Thoracic Society Research Statement. Am J Respir Crit Care Med. 2018;198:e15–e43. doi: 10.1164/rccm.201806-1160ST - DOI - PMC - PubMed
-
- Rain S, Bos Dda S, Handoko ML, Westerhof N, Stienen G, Ottenheijm C, Goebel M, Dorfmuller P, Guignabert C, Humbert M, et al. Protein changes contributing to right ventricular cardiomyocyte diastolic dysfunction in pulmonary arterial hypertension. J Am Heart Assoc. 2014;3:e000716. doi: 10.1161/JAHA.113.000716 - DOI - PMC - PubMed
-
- Hsu S, Kokkonen-Simon KM, Kirk JA, Kolb TM, Damico RL, Mathai SC, Mukherjee M, Shah AA, Wigley FM, Margulies KB, et al. Right Ventricular Myofilament Functional Differences in Humans With Systemic Sclerosis-Associated Versus Idiopathic Pulmonary Arterial Hypertension. Circulation. 2018;137:2360–2370. doi: 10.1161/CIRCULATIONAHA.117.033147 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
