

Antiplatelet therapy in aneurysmal subarachnoid hemorrhage: an updated meta-analysis
- PMID: 37665377
- PMCID: PMC10477151
- DOI: 10.1007/s10143-023-02120-2
Antiplatelet therapy in aneurysmal subarachnoid hemorrhage: an updated meta-analysis
Abstract
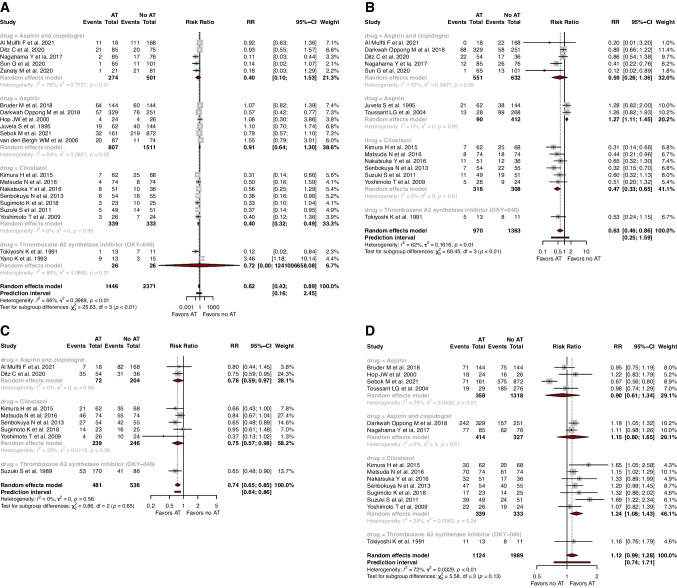
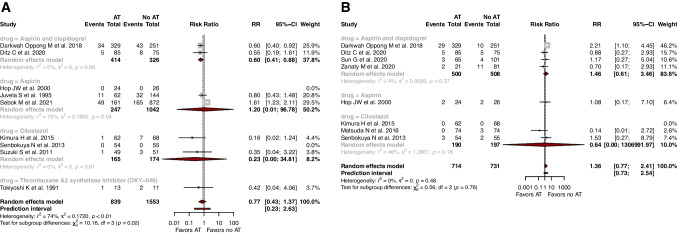
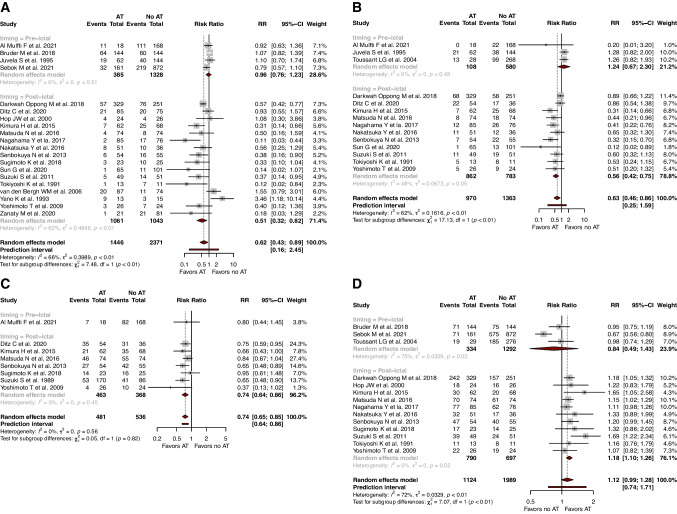
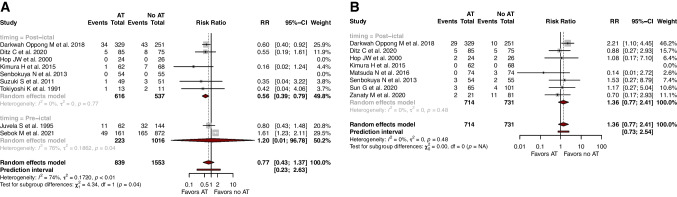
Antiplatelet therapy (AT) may serve to reduce the effects of aneurysmal subarachnoid hemorrhage (aSAH)-induced pro-coagulant state in the cerebral circulation. Several studies, however, have delivered conflicting conclusions on the efficacy of AT post aSAH. Systematic searches of Medline, Embase, and Cochrane Central were undertaken on 27th March 2023. The primary outcome was delayed cerebral ischaemia (DCI). Secondary outcomes were symptomatic and angiographic vasospasm, good functional outcome (modified Rankin Scale [mRS] with scores 0-2), hemorrhagic events, and in-hospital mortality. Twenty-two studies reporting 4378 patients with aSAH were included in the meta-analysis. AT was associated with lower rates of DCI (RR=0.62, 95% CI: 0.43; 0.89), symptomatic vasospasm (RR=0.63, 95% CI: 0.46; 0.86), and moderate/severe angiographic vasospasm (RR=0.74, 95% CI: 0.65; 0.84), with no effect on hemorrhagic complications (RR=1.36, 95% CI: 0.77; 2.41). When analyzing only post-ictal use of AT, AT additionally favored rates of good functional outcomes (RR=1.18, 95% CI: 1.10; 1.26) and in-hospital mortality (RR=0.56, 95% CI: 0.39; 0.80). In the subgroup treated with cilostazol, AT was associated with lower rates of DCI (RR=0.40, 95% CI: 0.32), symptomatic vasospasm (RR=0.47, 95% CI: 0.33; 0.65), moderate/severe angiographic vasospasm (RR=0.75, 95% CI: 0.57; 0.98) and good functional outcome (RR=1.24, 95% CI: 1.08; 1.43). In the surgically treated aSAH subgroup, AT favored rates of symptomatic vasospasm (RR=0.55, 95% CI: 0.30; 0.98), moderate/severe angiographic vasospasm (RR=0.70, 95% CI: 0.54; 0.90) and good functional outcome (RR=1.23, 95% CI: 1.09; 1.41). In the endovascularly treated aSAH subgroup, AT was associated with lower rates of in-hospital mortality (RR=0.60, 95% CI: 0.41; 0.88). In aSAH patients, post-ictal AT is associated with benefits in terms of rates of DCI, vasospasm, good functional outcomes, and in-hospital mortality without an increased risk of hemorrhagic events.
Keywords: Aneurysm; Antiplatelet; Ischemia; Meta-analysis; Neuroprotection; Stroke; Subarachnoid hemorrhage; Vasospasm.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
