

Vitamin D status and supplementation before and after Bariatric Surgery: Recommendations based on a systematic review and meta-analysis
- PMID: 37665480
- PMCID: PMC10698146
- DOI: 10.1007/s11154-023-09831-3
Vitamin D status and supplementation before and after Bariatric Surgery: Recommendations based on a systematic review and meta-analysis
Erratum in
-
Correction: Vitamin D status and supplementation before and after Bariatric Surgery: Recommendations based on a systematic review and meta‑analysis.Rev Endocr Metab Disord. 2024 Apr;25(2):447-448. doi: 10.1007/s11154-023-09837-x. Rev Endocr Metab Disord. 2024. PMID: 38502455 Free PMC article. No abstract available.
Abstract
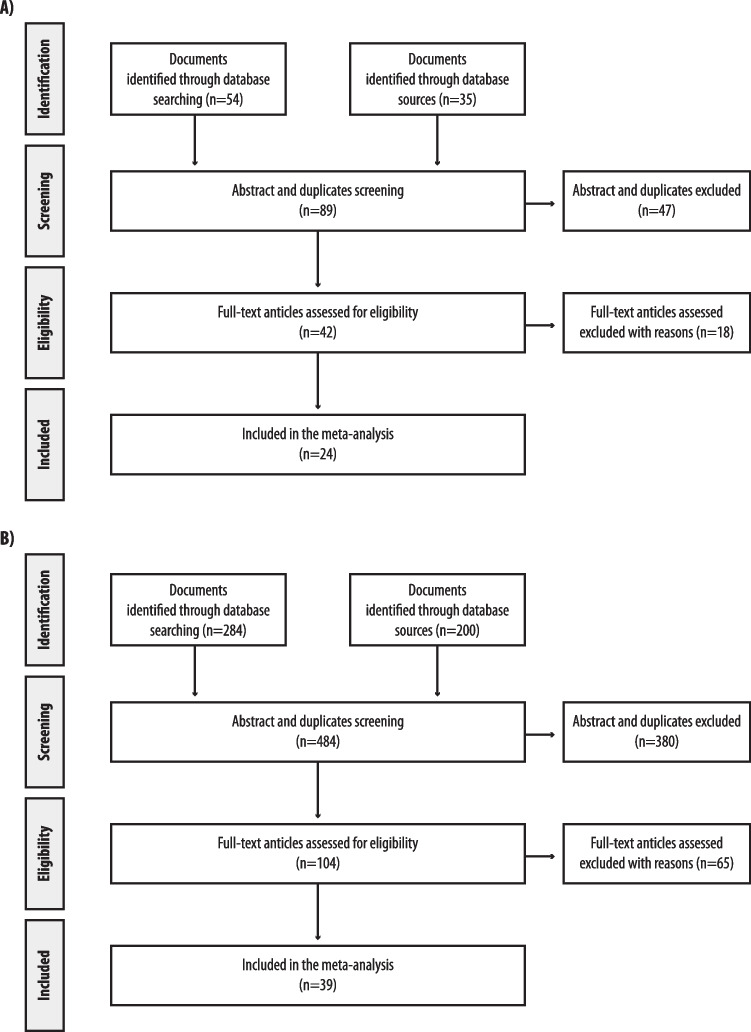
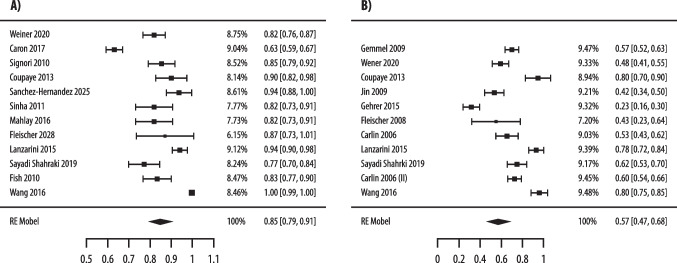
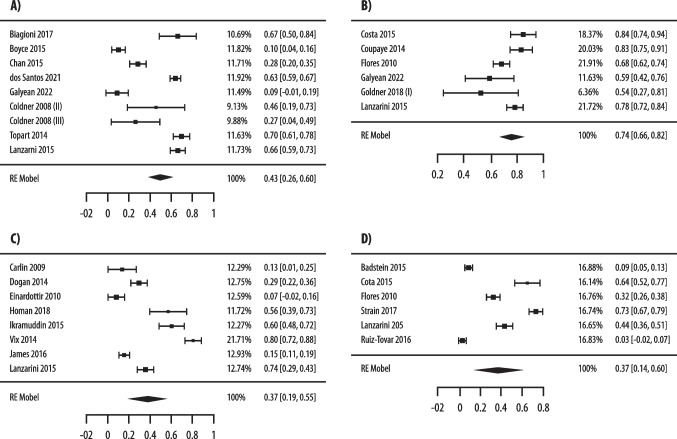
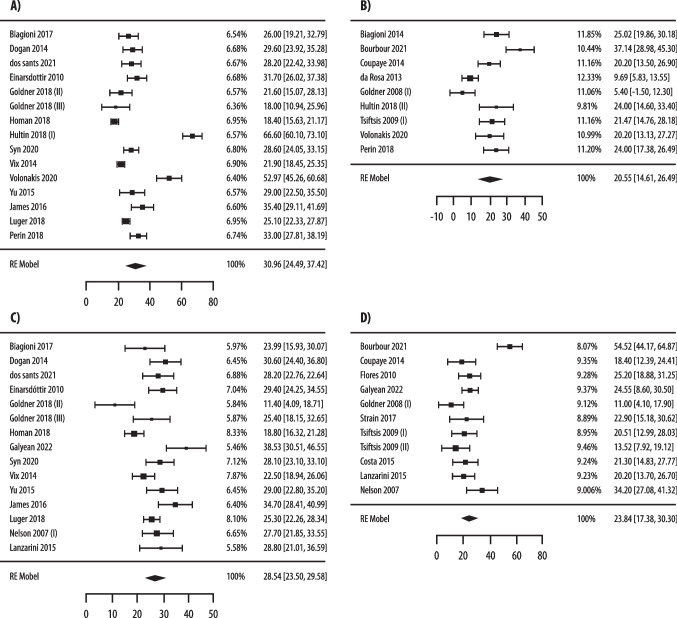
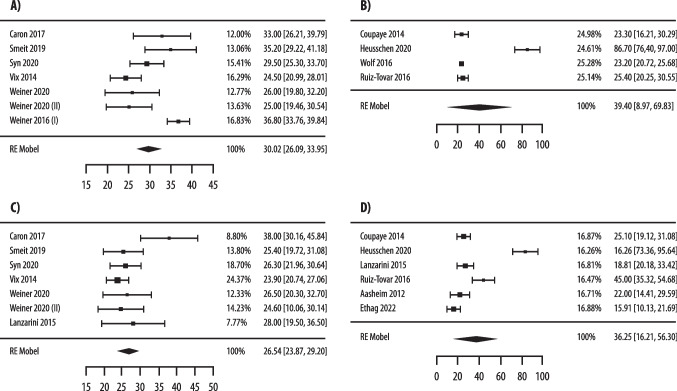
Bariatric surgery is associated with a postoperative reduction of 25(OH) vitamin D levels (25(OH)D) and with skeletal complications. Currently, guidelines for 25(OH)D assessment and vitamin D supplementation in bariatric patients, pre- and post-surgery, are still lacking. The aim of this work is to analyse systematically the published experience on 25(OH)D status and vitamin D supplementation, pre- and post-surgery, and to propose, on this basis, recommendations for management. Preoperatively, 18 studies including 2,869 patients were evaluated. Prevalence of vitamin D insufficiency as defined by 25(OH)D < 30 ng/mL (75 nmol/L) was 85%, whereas when defined by 25(OH)D < 20 ng/mL (50 nmol/L) was 57%. The median preoperative 25(OH)D level was 19.75 ng/mL. After surgery, 39 studies including 5,296 patients were analysed and among those undergoing either malabsorptive or restrictive procedures, a lower rate of vitamin D insufficiency and higher 25(OH)D levels postoperatively were observed in patients treated with high-dose oral vitamin D supplementation, defined as ≥ 2,000 IU/daily (mostly D3-formulation), compared with low-doses (< 2,000 IU/daily). Our recommendations based on this systematic review and meta-analysis should help clinical practice in the assessment and management of vitamin D status before and after bariatric surgery. Assessment of vitamin D should be performed pre- and postoperatively in all patients undergoing bariatric surgery. Regardless of the type of procedure, high-dose supplementation is recommended in patients after bariatric surgery.
Keywords: Bariatric surgery; Obesity; Vitamin D assay; Vitamin D insufficiency; Vitamin D supplementation.
© 2023. The Author(s).
Conflict of interest statement
L.D.F.; A.F.; R.A.; N.B; R.B.; F.F.C.; G.M.C.; M.C.; C.C.; L.M.D.; C.G.; G.L.; J.L.S.; C.S.; N.N.; J.K.V: no conflict of interest to declare.
Figures


References
-
- Ebeling PR, Adler RA, Jones G, et al. Management of endocrine disease: Therapeutics of Vitamin D. Eur J Endocrinol. 2018;179(5):R239–59. Published 2018 Oct 12. 10.1530/EJE-18-0151. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
