

First-line regorafenib with nivolumab and chemotherapy in advanced oesophageal, gastric, or gastro-oesophageal junction cancer in the USA: a single-arm, single-centre, phase 2 trial
- PMID: 37666264
- PMCID: PMC11208000
- DOI: 10.1016/S1470-2045(23)00358-3
First-line regorafenib with nivolumab and chemotherapy in advanced oesophageal, gastric, or gastro-oesophageal junction cancer in the USA: a single-arm, single-centre, phase 2 trial
Abstract
Background: The addition of nivolumab to chemotherapy improves survival in patients with advanced oesophagogastric (oesophageal, gastric, or gastro-oesophageal junction) adenocarcinoma; however, outcomes remain poor. We assessed the safety and activity of regorafenib in combination with nivolumab and chemotherapy in the first-line treatment of advanced oesophagogastric adenocarcinoma.
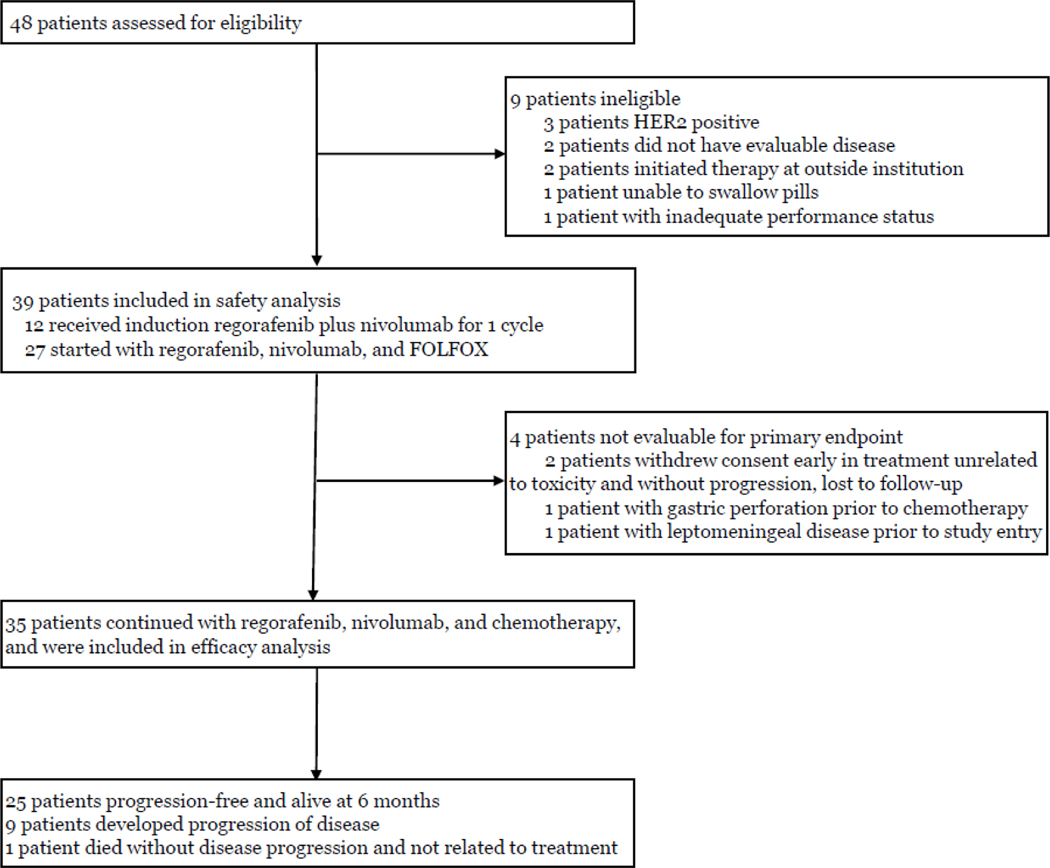
Methods: This investigator-initiated, single-arm, phase 2 trial in adult patients (aged ≥18 years) with previously untreated, HER2-negative, metastatic oesophagogastric adenocarcinoma was done at the Memorial Sloan Kettering Cancer Center (New York, NY, USA). Eligible patients had measurable disease or non-measurable disease that was evaluable (defined by Response Evaluation Criteria in Solid Tumours [RECIST] version 1.1) and Eastern Cooperative Oncology Group performance status of 0 or 1. Patients received FOLFOX chemotherapy (fluorouracil [400 mg/m2 bolus followed by 2400 mg/m2 over 48 h], leucovorin [400 mg/m2], and oxaliplatin [85 mg/m2]) and nivolumab (240 mg) intravenously on days 1 and 15, and oral regorafenib (80 mg) on days 1-21 of a 28-day cycle. Treatment was continued until disease progression (defined by RECIST version 1.1), unacceptable toxicity, or withdrawal of consent. The primary endpoint was 6-month progression-free survival in the per-protocol population (ie, all participants who received a dose of all study treatments). The regimen would be considered worthy of further investigation if at least 24 of 35 patients were progression free at 6 months. Safety was assessed in all participants who received at least one dose of any study treatment. This trial is registered with ClinicalTrials.gov, NCT04757363, and is now complete.
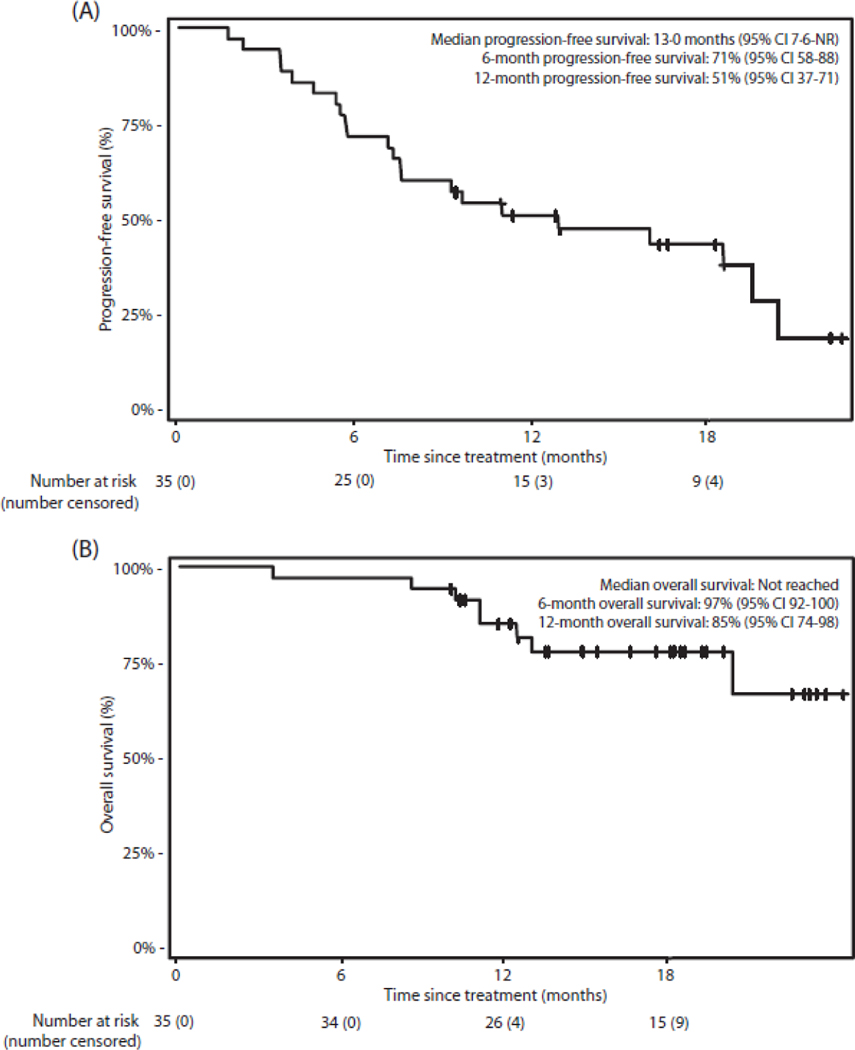
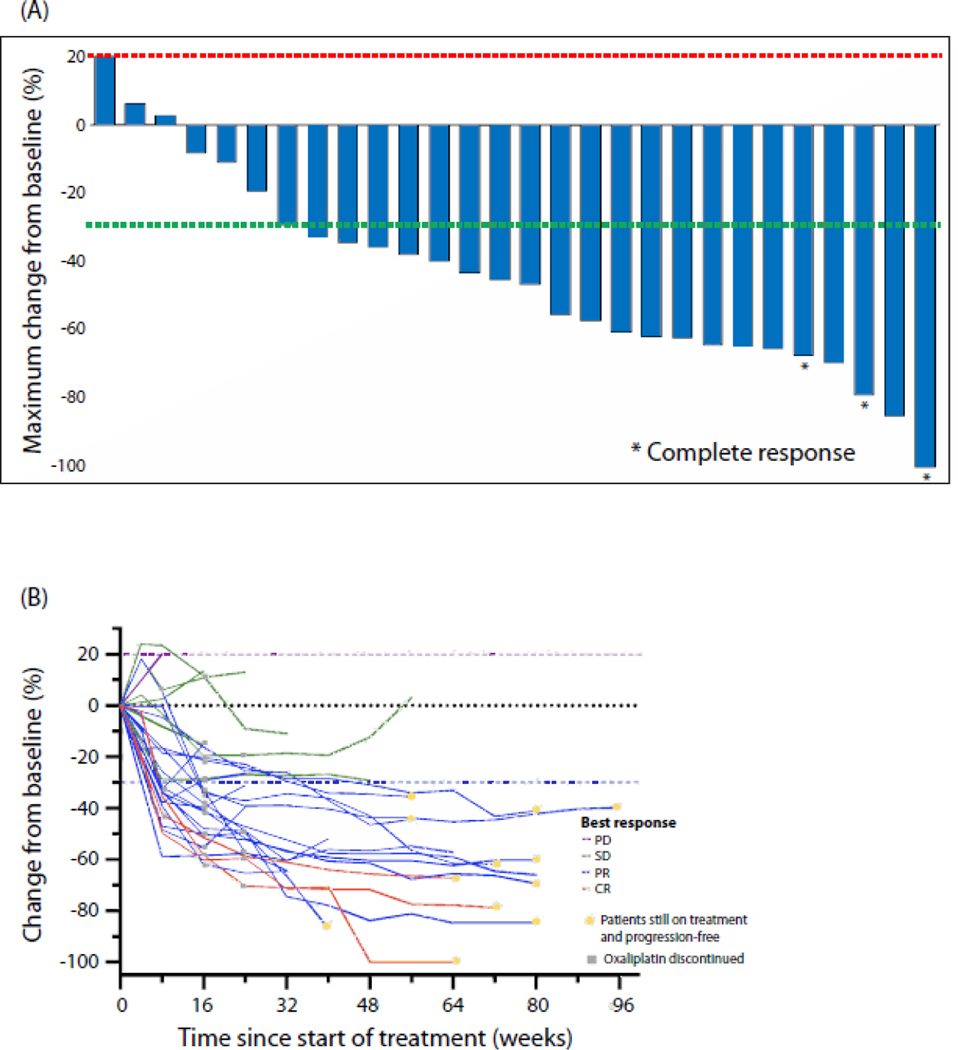
Findings: Between Feb 11, 2021, and May 4, 2022, 39 patients were enrolled, received at least one dose of study drug, and were included in safety analyses. 35 patients were evaluable for 6-month progression-free survival. Median age was 57 years (IQR 52-66), nine (26%) patients were women, 26 (74%) were men, 28 (80%) were White, and seven (20%) were Asian. At data cutoff (March 3, 2023), median follow-up was 18·1 months (IQR 12·7-20·4). The primary endpoint was reached, with 25 (71%; 95% CI 54-85) of 35 patients progression free at 6 months. Nine (26%) of 35 patients had disease progression and one (3%) patient died; the death was unrelated to treatment. The most common adverse event of any grade was fatigue (36 [92%] of 39). The most common grade 3 or 4 adverse events were decreased neutrophil count (18 [46%]), hypertension (six [15%]), dry skin, pruritus, or rash (five [13%]), and anaemia (four [10%]). Serious treatment-related adverse events occurred in ten (26%) patients, which were acute kidney injury (three [8%]), hepatotoxicity (two [5%]), sepsis (two [5%]), dry skin, pruritus, or rash (one [3%]), nausea (one [3%]), and gastric perforation (one [3%]). There were no treatment-related deaths.
Interpretation: Regorafenib can be safely combined with nivolumab and chemotherapy and showed promising activity in HER2-negative metastatic oesophagogastric cancer. A randomised, phase 3 clinical trial is planned.
Funding: Bristol Myers Squibb, Bayer and National Institutes of Health/National Cancer Institute.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SLC reports stock ownership in Pfizer, Moderna, and BioNTech. RHM reports consulting with PureTech Health, advisory board with IDEAYA Biosciences, and research funding from Nimbus Therapeutics. JFC reports an investigator role on a research study sponsored by Paige.AI. GYK reports consulting fees from AstraZeneca, Bristol-Myers Squibb, Merck, Pieris, and Zymeworks; and grants or contracts from AstraZeneca, Bristol-Myers Squibb, CARsgen, Zymeworks, Daiichi Sankyo, Oncolys, Pieris, and Adaptimmune. SBM reports honoraria from Natera, Bicara, Novartis, Basilea, Elevation Oncology, Purple Oncology, Pinetree Therapeutics, and Daiichi Sankyo; research support from Epic Sciences; grant funding from the Conquer Cancer Foundation; and research travel support from AstraZeneca outside of the submitted work. MAS reports consulting for Boston Scientific and Novo Nordisk. MEL reports ownership or equity interests with Apricity Health; intellectual property rights with John Wiley & Sons, and the Taylor & Francis Group; uncompensated provision of services for Oncoderm; and provision of services for Adgero Biopharmaceuticals, the American Academy of Dermatology, the American Society of Pediatric Hematology/Oncology, Apricity Health, AstraZeneca, Atlantic Canada Oncology Group, BGB Communications, Bicara Therapeutics, Deciphera, DelMar Pharmaceuticals, EMD Serono, GCO Global, Hoth Therapeutics, Incyte, Innovaderm Research, Johnson & Johnson, La Fonderie Ressources, La Roche-Posay, Loxo Oncology, Lutris Pharma, MJH Life Sciences, the Michigan Dermatological Society, NKMax America, NanOlogy, Novartis, Novartis Pharmaceuticals Corporation, Novocure, OnQuality Pharmaceuticals, Patient Resource, QED Therapeutics, RBC Consulting, RMEI Medical Education, Society for Immunotherapy of Cancer, Takeda Millennium, The Lynx Group, Tyra Biosciences, Varsona Pharmaceuticals, WebMD, Wolters Kluwer, and eSquared Communication Consulting. JS reports consulting for Paige.AI. MFB reports consulting for Eli Lilly and AstraZeneca (not related to this work). YYJ reports research funding from Bayer, Bristol Myers Squibb, Memorial Sloan Kettering Cancer Center Cycle for Survival, the United States Department of Defense, Eli Lilly, Fred's Team, Genentech/Roche, Merck, the National Cancer Institute, and RGENIX; advisory board or consulting with AbbVie, Amerisource Bergen, Ask-Gene Pharma, Arcus Biosciences, Astellas, Astra Zeneca, Basilea Pharmaceutica, Bayer, Bristol Myers Squibb, Clinical Care Options, Daiichi-Sankyo, Eli Lilly, Geneos Therapeutics, GlaxoSmithKline, Guardant Health, Imedex, Imugene, Lynx Health, Merck, Merck Serono, Mersana Therapeutics, Michael J Hennessy Associates, Paradigm Medical Communications, PeerView Institute, Pfizer, Research to Practice, RGENIX, Seagen, Silverback Therapeutics, and Zymeworks; and stock options in RGENIX. All other authors declare no competing interests.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022; 72(1): 7–33. - PubMed
-
- Sun JM, Shen L, Shah MA, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet 2021; 398(10302): 759–71. - PubMed
-
- Janjigian YY, Shitara K, Moehler MH, et al. Nivolumab plus chemotherapy vs chemo as first-line treatment for advanced gastric cancer/gastroesophageal junction cancer/esophageal adenocarcinoma: 3-year follow up from CheckMate 649 (Abstract No. LBA291, presented in oral format at the 2023 American Society of Clinical Oncology [ASCO] GI Cancers Symposium, January 19, 2023, San Francisco, CA). J Clin Oncol 2023; 41(Supplement 4, Abstract 291).
-
- Vesely MD, Zhang T, Chen L. Resistance Mechanisms to Anti-PD Cancer Immunotherapy. Annu Rev Immunol 2022; 40: 45–74. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
