

Predicted Impact of the Model for End-Stage Liver Disease 3.0 in a Region Suffering Severe Organ Shortage
- PMID: 37667579
- PMCID: PMC10477074
- DOI: 10.3346/jkms.2023.38.e274
Predicted Impact of the Model for End-Stage Liver Disease 3.0 in a Region Suffering Severe Organ Shortage
Abstract
Background: The model for end-stage liver disease 3.0 (MELD3.0) is expected to address the flaws of the current allocation system for deceased donor liver transplantation (DDLT). We aimed to validate MELD3.0 in the Korean population where living donor liver transplantation is predominant due to organ shortages.
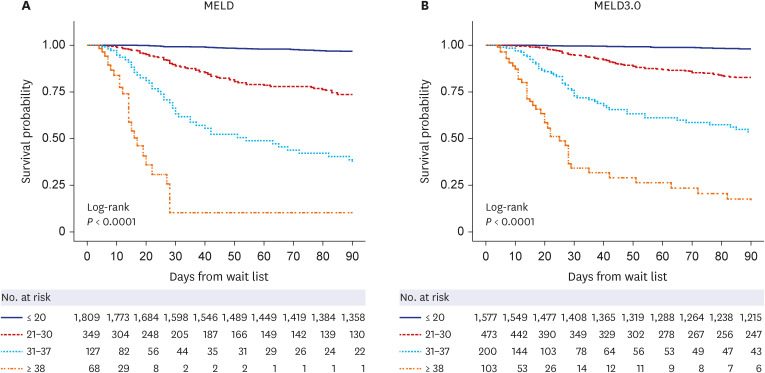
Methods: Korean large-volume single-centric waitlist data were merged with the Korean Network for Organ Sharing (KONOS) data. The 90-day mortality was compared between MELD and MELD3.0 using the C-index in 2,353 eligible patients registered for liver transplantation. Patient numbers and outcomes were compared based on changes in KONOS-MELD categorization using MELD3.0. Possible gains in MELD points and reduced waitlist mortality were analyzed.
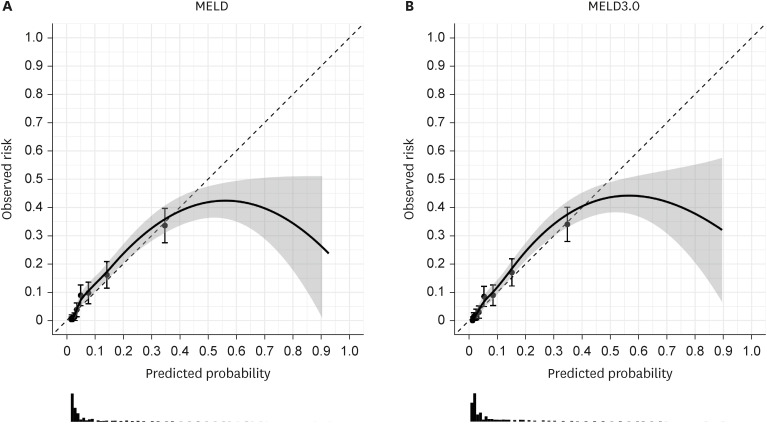
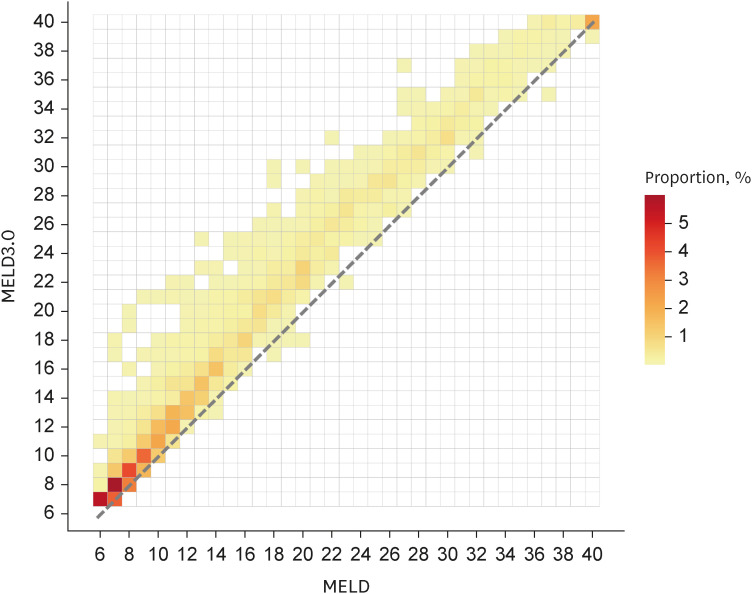
Results: MELD3.0 performed better than MELD (C-index 0.893 for MELD3.0 vs. 0.889 for MELD). When stratified according to the KONOS-MELD categories, 15.9% of the total patients and 35.2% of the deceased patients were up-categorized using MELD3.0 versus MELD categories. The mean gain of MELD points was higher in women (2.6 ± 2.1) than men (2.1 ± 1.9, P < 0.001), and higher in patients with severe ascites (3.3 ± 1.8) than in controls (1.9 ± 1.8, P < 0.001); however, this trend was not significant when the MELD score was higher than 30. When the possible increase in DDLT chance was calculated via up-categorizing using MELD3.0, reducible waitlist mortality was 2.7%.
Conclusion: MELD3.0 could predict better waitlist mortality than MELD; however, the merit for women and patients with severe ascites is uncertain, and reduced waitlist mortality from implementing MELD3.0 is limited in regions suffering from organ shortage, as in Korea.
Keywords: Allocation; Liver Transplantation; MELD; MELD3.0; Waitlist Mortality.
© 2023 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33(2):464–470. - PubMed
-
- Nagai S, Chau LC, Schilke RE, Safwan M, Rizzari M, Collins K, et al. Effects of allocating livers for transplantation based on model for end-stage liver disease-sodium scores on patient outcomes. Gastroenterology. 2018;155(5):1451–1462.e3. - PubMed
-
- Godfrey EL, Malik TH, Lai JC, Mindikoglu AL, Galván NT, Cotton RT, et al. The decreasing predictive power of MELD in an era of changing etiology of liver disease. Am J Transplant. 2019;19(12):3299–3307. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
