

Intensive vs Conventional Blood Pressure Lowering After Endovascular Thrombectomy in Acute Ischemic Stroke: The OPTIMAL-BP Randomized Clinical Trial
- PMID: 37668619
- PMCID: PMC10481233
- DOI: 10.1001/jama.2023.14590
Intensive vs Conventional Blood Pressure Lowering After Endovascular Thrombectomy in Acute Ischemic Stroke: The OPTIMAL-BP Randomized Clinical Trial
Abstract
Importance: Optimal blood pressure (BP) control after successful reperfusion with endovascular thrombectomy (EVT) for patients with acute ischemic stroke is unclear.
Objective: To determine whether intensive BP management during the first 24 hours after successful reperfusion leads to better clinical outcomes than conventional BP management in patients who underwent EVT.
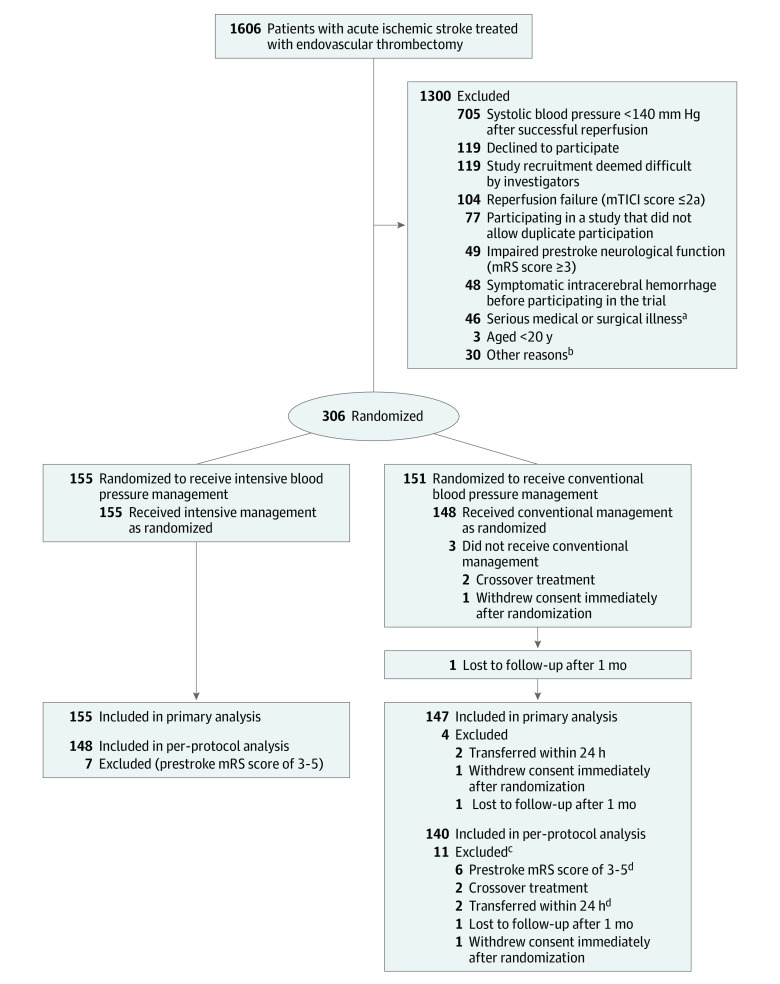
Design, setting, and participants: Multicenter, randomized, open-label trial with a blinded end-point evaluation, conducted across 19 stroke centers in South Korea from June 2020 to November 2022 (final follow-up, March 8, 2023). It included 306 patients with large vessel occlusion acute ischemic stroke treated with EVT and with a modified Thrombolysis in Cerebral Infarction score of 2b or greater (partial or complete reperfusion).
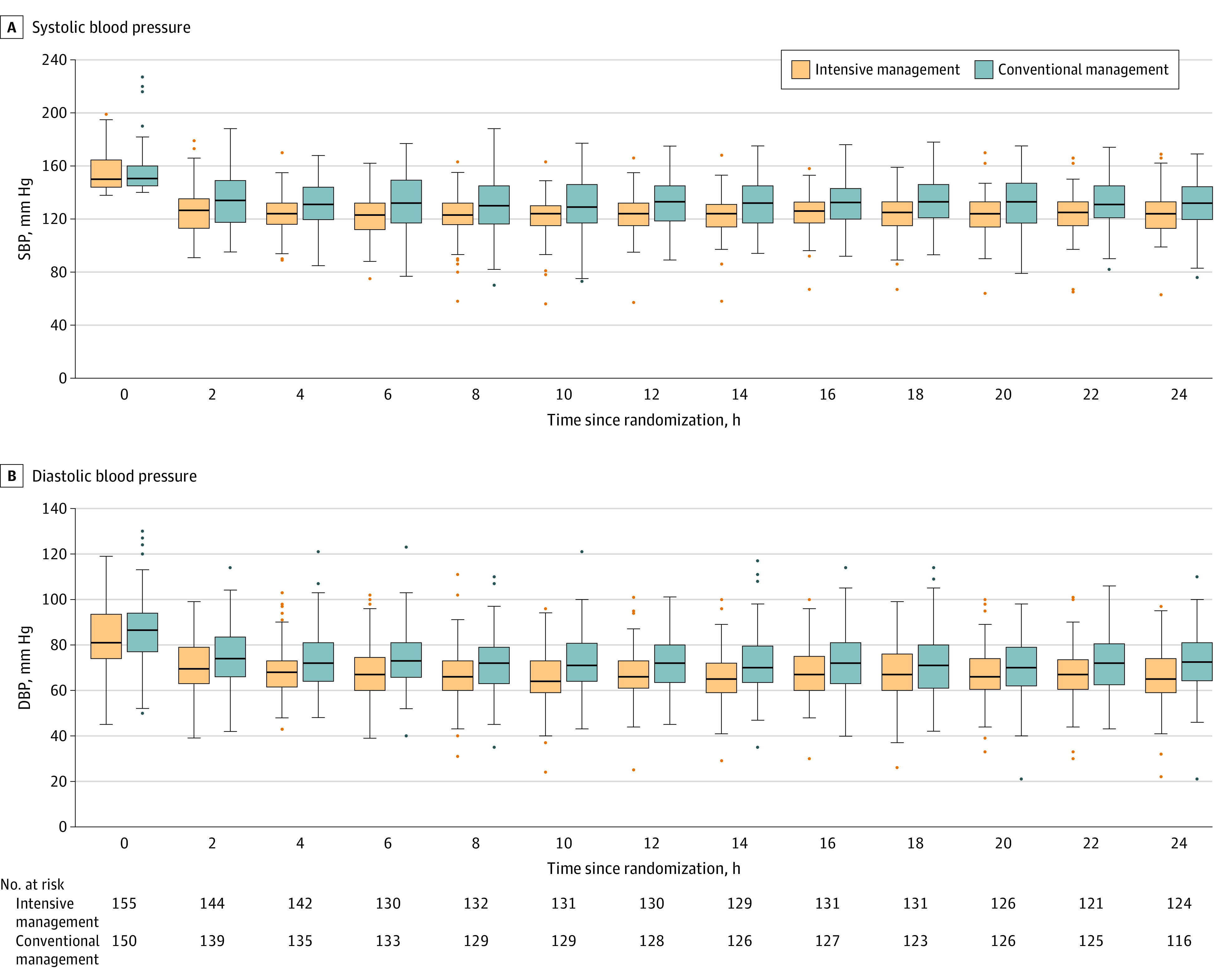
Interventions: Participants were randomly assigned to receive intensive BP management (systolic BP target <140 mm Hg; n = 155) or conventional management (systolic BP target 140-180 mm Hg; n = 150) for 24 hours after enrollment.
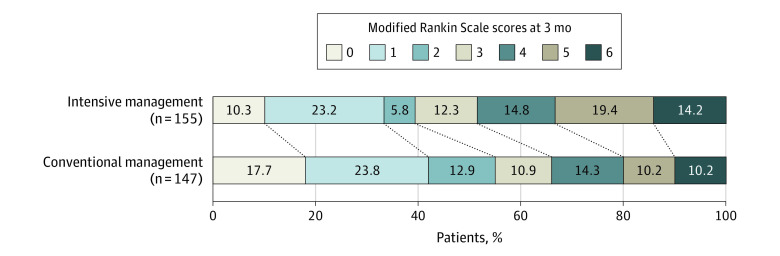
Main outcomes and measures: The primary outcome was functional independence at 3 months (modified Rankin Scale score of 0-2). The primary safety outcomes were symptomatic intracerebral hemorrhage within 36 hours and death related to the index stroke within 3 months.
Results: The trial was terminated early based on the recommendation of the data and safety monitoring board, which noted safety concerns. Among 306 randomized patients, 305 were confirmed eligible and 302 (99.0%) completed the trial (mean age, 73.0 years; 122 women [40.4%]). The intensive management group had a lower proportion achieving functional independence (39.4%) than the conventional management group (54.4%), with a significant risk difference (-15.1% [95% CI, -26.2% to -3.9%]) and adjusted odds ratio (0.56 [95% CI, 0.33-0.96]; P = .03). Rates of symptomatic intracerebral hemorrhage were 9.0% in the intensive group and 8.1% in the conventional group (risk difference, 1.0% [95% CI, -5.3% to 7.3%]; adjusted odds ratio, 1.10 [95% CI, 0.48-2.53]; P = .82). Death related to the index stroke within 3 months occurred in 7.7% of the intensive group and 5.4% of the conventional group (risk difference, 2.3% [95% CI, -3.3% to 7.9%]; adjusted odds ratio, 1.73 [95% CI, 0.61-4.92]; P = .31).
Conclusions and relevance: Among patients who achieved successful reperfusion with EVT for acute ischemic stroke with large vessel occlusion, intensive BP management for 24 hours led to a lower likelihood of functional independence at 3 months compared with conventional BP management. These results suggest that intensive BP management should be avoided after successful EVT in acute ischemic stroke.
Trial registration: ClinicalTrials.gov Identifier: NCT04205305.
Conflict of interest statement
Figures
Comment in
-
Blood Pressure Management After Successful Thrombectomy.JAMA. 2023 Sep 5;330(9):811-812. doi: 10.1001/jama.2023.14588. JAMA. 2023. PMID: 37668632 No abstract available.
-
After EVT for ischemic stroke, intensive vs. conventional BP management reduced functional independence at 3 mo.Ann Intern Med. 2024 Jan;177(1):JC5. doi: 10.7326/J23-0106. Epub 2024 Jan 2. Ann Intern Med. 2024. PMID: 38163376
References
-
- Lapergue B, Blanc R, Costalat V, et al. ; ASTER2 Trial Investigators . Effect of thrombectomy with combined contact aspiration and stent retriever vs stent retriever alone on revascularization in patients with acute ischemic stroke and large vessel occlusion: the ASTER2 randomized clinical trial. JAMA. 2021;326(12):1158-1169. doi: 10.1001/jama.2021.13827 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
