

The Pivotal Role of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers in Hypertension Management and Cardiovascular and Renal Protection: A Critical Appraisal and Comparison of International Guidelines
- PMID: 37668854
- PMCID: PMC10625506
- DOI: 10.1007/s40256-023-00605-5
The Pivotal Role of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers in Hypertension Management and Cardiovascular and Renal Protection: A Critical Appraisal and Comparison of International Guidelines
Abstract
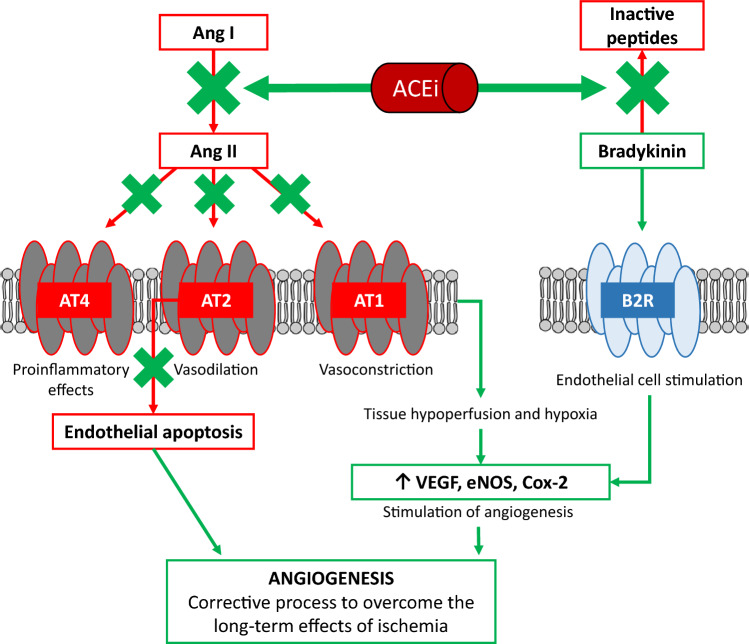
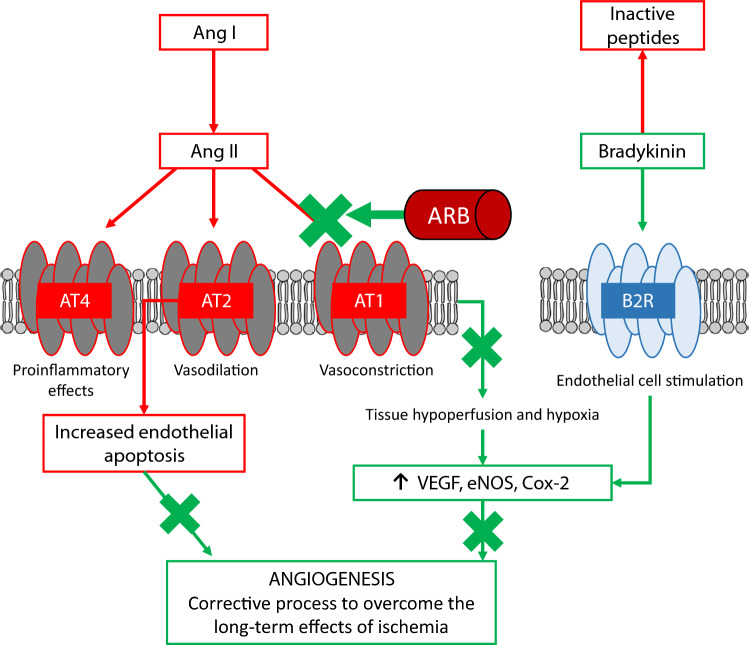
Arterial hypertension is the main preventable cause of premature mortality worldwide. Across Latin America, hypertension has an estimated prevalence of 25.5-52.5%, although many hypertensive patients remain untreated. Appropriate treatment, started early and continued for the remaining lifespan, significantly reduces the risk of complications and mortality. All international and most regional guidelines emphasize a central role for renin-angiotensin-aldosterone system inhibitors (RAASis) in antihypertensive treatment. The two main RAASi options are angiotensin-converting enzyme inhibitors (ACEis) and angiotensin II receptor blockers (ARBs). Although equivalent in terms of blood pressure reduction, ACEis are preferably recommended by some guidelines to manage other cardiovascular comorbidities, with ARBs considered as an alternative when ACEis are not tolerated. This review summarizes the differences between ACEis and ARBs and their place in the international guidelines. It provides a critical appraisal of the guidelines based on available evidence from randomized controlled trials (RCTs) and meta-analyses, especially considering that hypertensive patients in daily practice often have other comorbidities. The observed differences in cardiovascular and renal outcomes in RCTs may be attributed to the different mechanisms of action of ACEis and ARBs, including increased bradykinin levels, potentiated bradykinin response, and stimulated nitric oxide production with ACEis. It may therefore be appropriate to consider ACEis and ARBs as different antihypertensive drugs classes within the same RAASi group. Although guideline recommendations only differentiate between ACEis and ARBs in patients with cardiovascular comorbidities, clinical evidence suggests that ACEis provide benefits in many hypertensive patients, as well as those with other cardiovascular conditions.
© 2023. The Author(s).
Conflict of interest statement
Luis Alcocer: Honoraria as consultant from MSD, Menarini, Novartis, Pfizer, Sanofi-Aventis, Servier, Silanes, Stendhal, Takeda, and Viatris; honoraria for presentations and involvement in educational seminars from Asofarma, AstraZeneca, Bayer, Daichi-Sankyo, MSD, Menarini, Novartis, Pfizer, Sanofi-Aventis, Servier, Silanes, Stendhal, Takeda, and Viatris. Alfonso Bryce: Honoraria for lectures from Abbott, AstraZeneca, Bayer, Biotoscana, Boehringer Ingelheim, Bristol Myers Squibb, Emcure, Farmakonsuma, Farmindustria, GlaxoSmithKline, Grupo Farma, Megalabs, Menarini, Merck Serono, MSD, Novartis, OM Pharma, Pfizer, Roemmers, Sanofi-Aventis, Servier, Schering-Plough, Tecnofarma, and Teva; research grants from Abbott, GlaxoSmithKline, MSD, Novartis, and Takeda; personal fees for advisory board participation from Abbott, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, MSD, Novartis, and Pfizer; and honoraria as consultant from Servier. David de Padua Brasil: Served as the NLI (Brazil) and reports institutional grants from Bayer during the conduct of the Voyager PAD clinical trial; honoraria as consultant from Servier and Libbs; personal fees to write scientific educational materials, participate in scientific boards, and speak in educational meetings/seminars from Libbs and Servier; travel grants to cover transport, hotel accommodations, and registration fee to attend international educational congresses from Servier; and personal fees to speak at scientific meetings organized/sponsored by Viatris, Biolab, Bayer, and Bristol Myers Squibb. Joffre Lara: Honoraria for presentations and involvement in educational seminars from Servier, Astra Zeneca, Novartis, Boehringer Ingelheim, Novo Nordisk, Merck, Medicamenta, and Megalabs. Javier Moreno Cortes: Honoraria for presentations and involvement in educational seminars from Servier. Daniel Quesada: Honoraria for presentations and involvement in educational seminars from Servier, AstraZeneca, Pfizer, and Novartis; consultation fees from Pfizer, Servier, AstraZeneca, and Merck; and educational and travel grants from Bayer, Ferrer, and Astra Zeneca. Pablo Rodriguez: Honoraria for consultations, presentations, and involvement in educational seminars from Servier, Bagó, Baliarda, Gador, and Raffo; and travel grants from Servier, Bagó, and Baliarda.
Figures
Similar articles
-
Updates on the treatment of essential hypertension: a summary of AHRQ's comparative effectiveness review of angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and direct renin inhibitors.J Manag Care Pharm. 2011 Oct;17(8 Suppl):S1-14. doi: 10.18553/jmcp.2011.17.s8.1. J Manag Care Pharm. 2011. PMID: 22088101 Free PMC article. Review.
-
The benefits of angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers combined with calcium channel blockers on metabolic, renal, and cardiovascular outcomes in hypertensive patients: a meta-analysis.Int Urol Nephrol. 2018 Dec;50(12):2261-2278. doi: 10.1007/s11255-018-1991-x. Epub 2018 Oct 15. Int Urol Nephrol. 2018. PMID: 30324578
-
Association Between Renin-Angiotensin-Aldosterone System Inhibitors and Clinical Outcomes in Patients With COVID-19: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Mar 1;4(3):e213594. doi: 10.1001/jamanetworkopen.2021.3594. JAMA Netw Open. 2021. PMID: 33787911 Free PMC article.
-
Renin Angiotensin Blockers and Cardiac Protection: From Basis to Clinical Trials.Am J Hypertens. 2022 Apr 2;35(4):293-302. doi: 10.1093/ajh/hpab108. Am J Hypertens. 2022. PMID: 34265036 Review.
-
Angiotensin Receptor Blockers Versus Angiotensin Converting Enzyme Inhibitors for the Treatment of Arterial Hypertension and the Role of Olmesartan.Adv Ther. 2019 Feb;36(2):278-297. doi: 10.1007/s12325-018-0859-x. Epub 2018 Dec 27. Adv Ther. 2019. PMID: 30591990 Free PMC article. Review.
Cited by
-
The Interplay of Heart Failure and Lung Disease: Clinical Correlations, Mechanisms, and Therapeutic Implications.J Respir Biol Transl Med. 2024 Dec;1(4):10020. doi: 10.70322/jrbtm.2024.10020. Epub 2024 Dec 2. J Respir Biol Transl Med. 2024. PMID: 39916950 Free PMC article.
-
Gut Microbiota and Cardiovascular Diseases: Unraveling the Role of Dysbiosis and Microbial Metabolites.Int J Mol Sci. 2025 Apr 30;26(9):4264. doi: 10.3390/ijms26094264. Int J Mol Sci. 2025. PMID: 40362500 Free PMC article. Review.
-
Functional and Bioactive Benefits of Selected Microalgal Hydrolysates Assessed In Silico and In Vitro.Mar Drugs. 2025 Jan 22;23(2):53. doi: 10.3390/md23020053. Mar Drugs. 2025. PMID: 39997177 Free PMC article.
-
Drug-Induced Myocardial Infarction: A Review of Pharmacological Triggers and Pathophysiological Mechanisms.J Cardiovasc Dev Dis. 2024 Dec 18;11(12):406. doi: 10.3390/jcdd11120406. J Cardiovasc Dev Dis. 2024. PMID: 39728296 Free PMC article. Review.
-
Ile-Pro-Pro attenuates sympathetic activity and hypertension.J Physiol Biochem. 2024 Aug;80(3):585-598. doi: 10.1007/s13105-024-01034-x. Epub 2024 Jul 15. J Physiol Biochem. 2024. PMID: 39008241
References
-
- NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi: 10.1016/S0140-6736(21)01330-1. - DOI - PMC - PubMed
-
- Blood Pressure Lowering Treatment Trialists Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet. 2021;397(10285):1625–36. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
