

Prevention of Radiographic Progression in Higher-Risk Patients with Rheumatoid Arthritis Using Filgotinib in Phase III Studies: Narrative Review of Post Hoc Analyses
- PMID: 37668865
- PMCID: PMC10654325
- DOI: 10.1007/s40744-023-00590-w
Prevention of Radiographic Progression in Higher-Risk Patients with Rheumatoid Arthritis Using Filgotinib in Phase III Studies: Narrative Review of Post Hoc Analyses
Abstract
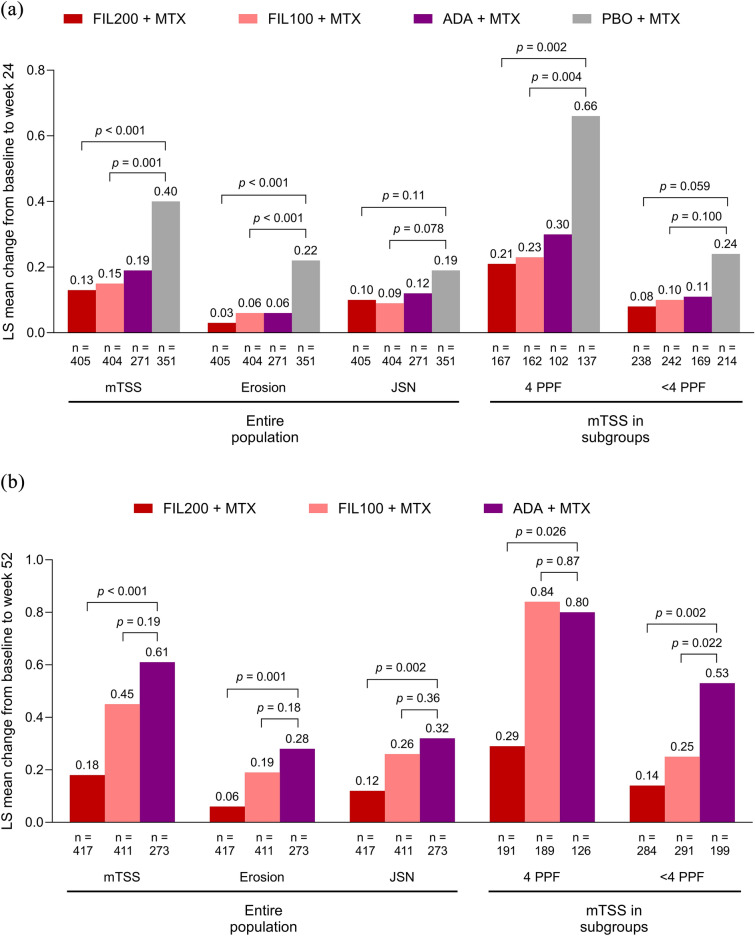
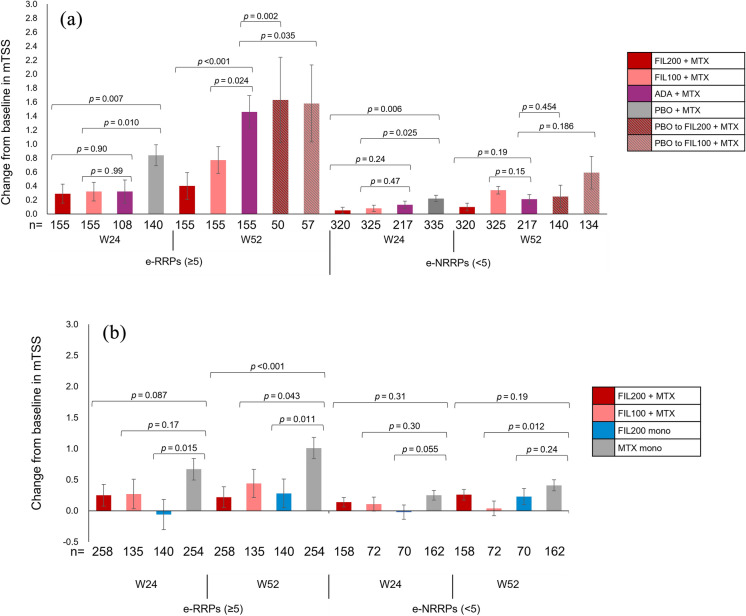
Filgotinib is an oral preferential Janus kinase 1 inhibitor that demonstrated significant reductions in radiographic progression, with an acceptable tolerability and safety profile, vs placebo in patients with rheumatoid arthritis (RA) and an inadequate response to methotrexate (MTX-IR; FINCH 1) and vs MTX in MTX-naïve patients with RA (FINCH 3). International treatment guidelines identify multiple poor prognostic factors (PPFs) associated with worse disease outcomes among patients with RA. However, questions remain both about the clinical utility of considering PPFs and about which PPFs should drive treatment decisions. Additionally, the role of radiographic findings in clinical practice continues to be discussed and to evolve. This review examines radiographic results from post hoc analyses of phase 3 trials of filgotinib that examined subgroups with 4 PPFs or with baseline estimated rapid radiographic progression (e-RRP). In MTX groups, there were trends toward greater progression among patients with 4 PPFs or e-RRP, suggesting these subgroups may comprise a higher-risk population. Results show general consistency for the efficacy of filgotinib 200 mg plus MTX vs placebo plus MTX/MTX monotherapy on radiographic assessments, including change from baseline in modified total Sharp score and proportions without radiographic progression, even among MTX-IR or MTX-naïve patients with 4 PPFs or e-RRP who may be at higher risk of bone damage. Multivariate analysis identified multiple factors associated with baseline e-RRP status. This summary of the current understanding of benefits associated with filgotinib on radiographic progression and the relevance of baseline factors to these benefits may help inform treatment decisions for patients facing high risk of radiographic progression.
Keywords: Adalimumab; Filgotinib; Methotrexate; Poor prognostic factors; Rheumatoid arthritis.
© 2023. The Author(s).
Conflict of interest statement
Yoshiya Tanaka received speaking fees and/or honoraria from AbbVie, Amgen, Astellas, AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Chugai, Eisai, Eli Lilly, Gilead, Mitsubishi-Tanabe, and YL Biologics and received research grants from AbbVie, Asahi-Kasei, Boehringer-Ingelheim, Chugai, Corrona, Daiichi Sankyo, Eisai, Kowa, Mitsubishi-Tanabe, and Takeda. Tsutomu Takeuchi reports receiving grant/research support from AbbVie, Asahi Kasei, Astellas, Chugai, Daiichi Sankyo, Eisai, Mitsubishi-Tanabe, Shionogi, Takeda, and UCB Japan; serving as a consultant for Astellas, Chugai, and Eli Lilly Japan; and serving on a speakers’ bureau for AbbVie, Ayumi Pharmaceutical Corporation, Bristol-Myers Squibb, Chugai, Daiichi Sankyo, Dainippon Sumitomo Eisai, Eli Lilly Japan, Mitsubishi-Tanabe, Novartis, Pfizer Japan, Sanofi, and Gilead Sciences, Inc. Tatsuya Atsumi received research grants, speaking fees, and/or consultancy fees from Gilead Sciences K.K.; Eisai Co., Ltd.; AbbVie Inc.; Alexion Inc.; Asahi-Kasei Co.; Astellas Pharma Inc.; AstraZeneca plc.; Bayer Yakuhin; Bristol-Myers Squibb Co.; Chugai Pharmaceutical Co., Ltd.; Daiichi Sankyo Co., Ltd.; Eli Lilly Japan K.K.; GlaxoSmithKline K.K.; Janssen Pharmaceutical K.K.; Kyowa Kirin Co., Ltd.; Novartis Pharma K.K.; Nippon Boehringer Ingelheim Co., Ltd.; Mitsubishi Tanabe Pharma Co.; Ono Pharmaceutical Co. Ltd.; Otsuka Pharmaceutical Co., Ltd.; Pfizer Inc.; Taiho Pharmaceutical Co., Ltd.; Takeda Pharmaceutical Co., Ltd.; Teijin Pharma Ltd.; and UCB Japan Co. Ltd. Bernard G. Combe receives grant/research support from Pfizer and Roche-Chugai; and received consulting and/or speaker fees from AbbVie, Bristol-Myers Squibb, Celltrion, Eli Lilly, Gilead-Galapagos, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, and Roche-Chugai. Daniel Aletaha reports grants or research support from AbbVie, Merck Sharp & Dohme, Novartis, and Roche; serving as a consultant for Janssen; serving on a speaker’s bureau for Bristol-Myers Squibb, Merck Sharp & Dohme, and UCB; and serving as a consultant and on a speaker’s bureau for AbbVie, Amgen, Celgene, Eli Lilly, Medac, Merck, Novartis, Pfizer, Roche, Sandoz, and Sanofi/Genzyme. Toshihiko Kaise is an employee of Gilead Sciences K.K. and shareholder of Gilead Sciences, Inc. Vijay Rajendran is an employee and shareholder of Galapagos BV.
Figures


Similar articles
-
Filgotinib Radiographic and Clinical Efficacy Versus Other JAK Inhibitors and Adalimumab in Patients With Rheumatoid Arthritis and Inadequate Response to Methotrexate: A Systematic Review and Network Meta-Analysis.Rheumatol Ther. 2025 Jun;12(3):453-468. doi: 10.1007/s40744-025-00757-7. Epub 2025 Apr 10. Rheumatol Ther. 2025. PMID: 40208566 Free PMC article. Review.
-
Benefit of Filgotinib, a JAK1 Preferential Inhibitor, in Rheumatoid Arthritis Patients with Previous Rapid Radiographic Progression: Post Hoc Analysis of Two Trials.Rheumatol Ther. 2023 Feb;10(1):161-185. doi: 10.1007/s40744-022-00503-3. Epub 2022 Nov 3. Rheumatol Ther. 2023. PMID: 36327094 Free PMC article.
-
Efficacy and safety of filgotinib in methotrexate-naive patients with rheumatoid arthritis with poor prognostic factors: post hoc analysis of FINCH 3.RMD Open. 2021 Aug;7(2):e001621. doi: 10.1136/rmdopen-2021-001621. RMD Open. 2021. PMID: 34385364 Free PMC article. Clinical Trial.
-
Efficacy and Safety of Filgotinib in Patients with High Risk of Poor Prognosis Who Showed Inadequate Response to MTX: A Post Hoc Analysis of the FINCH 1 Study.Rheumatol Ther. 2023 Feb;10(1):53-70. doi: 10.1007/s40744-022-00498-x. Epub 2022 Oct 9. Rheumatol Ther. 2023. PMID: 36209441 Free PMC article.
-
Long-Term Safety, Efficacy, and Patient-Centered Outcomes of Filgotinib in the Treatment of Rheumatoid Arthritis: Current Perspectives.Patient Prefer Adherence. 2023 Oct 6;17:2499-2516. doi: 10.2147/PPA.S417677. eCollection 2023. Patient Prefer Adherence. 2023. PMID: 37822545 Free PMC article. Review.
Cited by
-
The Uncoupling of Disease Activity from Joint Structural Progression in Patients with Rheumatoid Arthritis Treated with Filgotinib.Rheumatol Ther. 2025 Feb;12(1):53-66. doi: 10.1007/s40744-024-00725-7. Epub 2024 Nov 26. Rheumatol Ther. 2025. PMID: 39592547 Free PMC article.
-
Filgotinib Radiographic and Clinical Efficacy Versus Other JAK Inhibitors and Adalimumab in Patients With Rheumatoid Arthritis and Inadequate Response to Methotrexate: A Systematic Review and Network Meta-Analysis.Rheumatol Ther. 2025 Jun;12(3):453-468. doi: 10.1007/s40744-025-00757-7. Epub 2025 Apr 10. Rheumatol Ther. 2025. PMID: 40208566 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
