

Comorbidity Patterns in Patients Newly Diagnosed With Colorectal Cancer: Network-Based Study
- PMID: 37669093
- PMCID: PMC10509734
- DOI: 10.2196/41999
Comorbidity Patterns in Patients Newly Diagnosed With Colorectal Cancer: Network-Based Study
Abstract
Background: Patients with colorectal cancer (CRC) often present with multiple comorbidities, and many of these can affect treatment and survival. However, previous comorbidity studies primarily focused on diseases in commonly used comorbidity indices. The comorbid status of CRC patients with respect to the entire spectrum of chronic diseases has not yet been investigated.
Objective: This study aimed to systematically analyze all chronic diagnoses and diseases co-occurring, using a network-based approach and large-scale administrative health data, and provide a complete picture of the comorbidity pattern in patients newly diagnosed with CRC from southwest China.
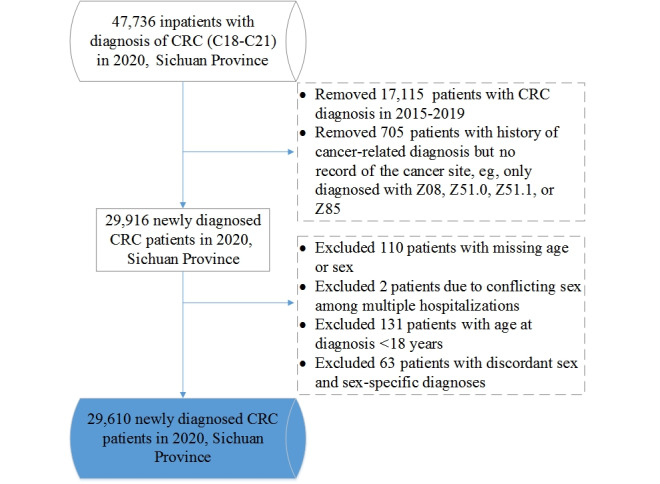
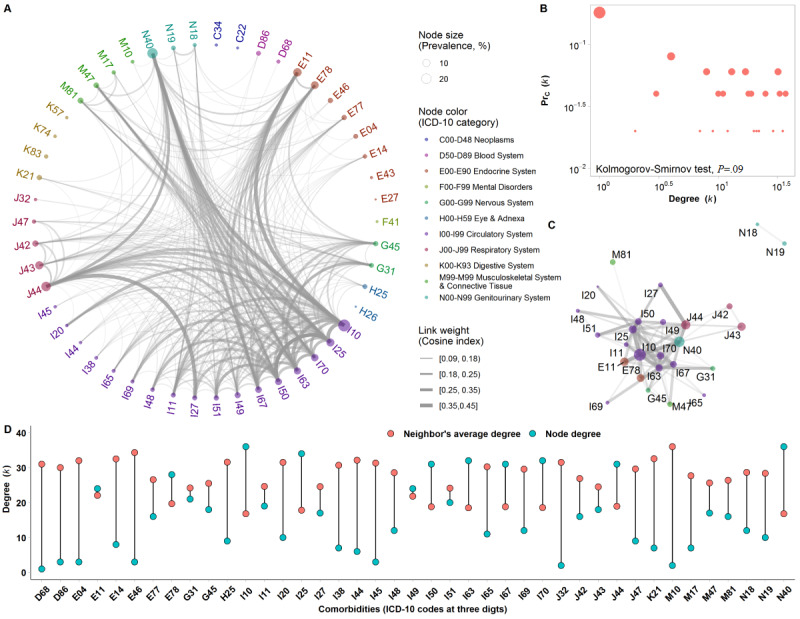
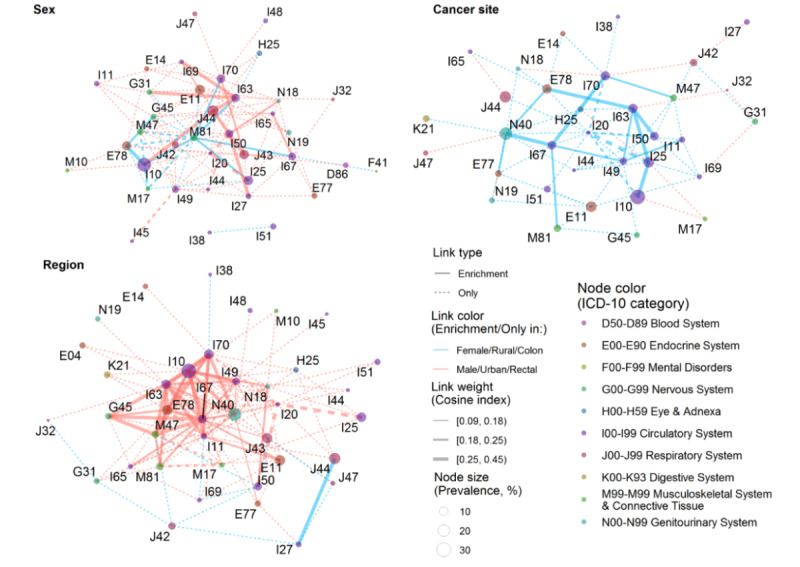
Methods: In this retrospective observational study, the hospital discharge records of 678 hospitals from 2015 to 2020 in Sichuan Province, China were used to identify new CRC cases in 2020 and their history of diseases. We examined all chronic diagnoses using ICD-10 (International Classification of Diseases, 10th Revision) codes at 3 digits and focused on chronic diseases with >1% prevalence in at least one subgroup (1-sided test, P<.025), which resulted in a total of 66 chronic diseases. Phenotypic comorbidity networks were constructed across all CRC patients and different subgroups by sex, age (18-59, 60-69, 70-79, and ≥80 years), area (urban and rural), and cancer site (colon and rectum), with comorbidity as a node and linkages representing significant correlations between multiple comorbidities.
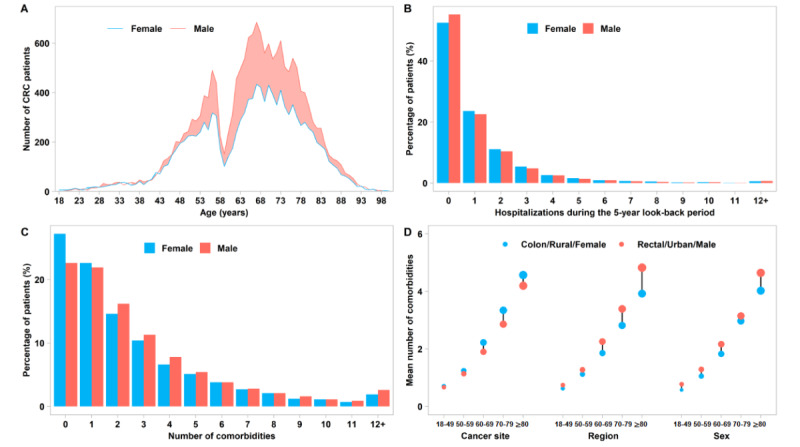
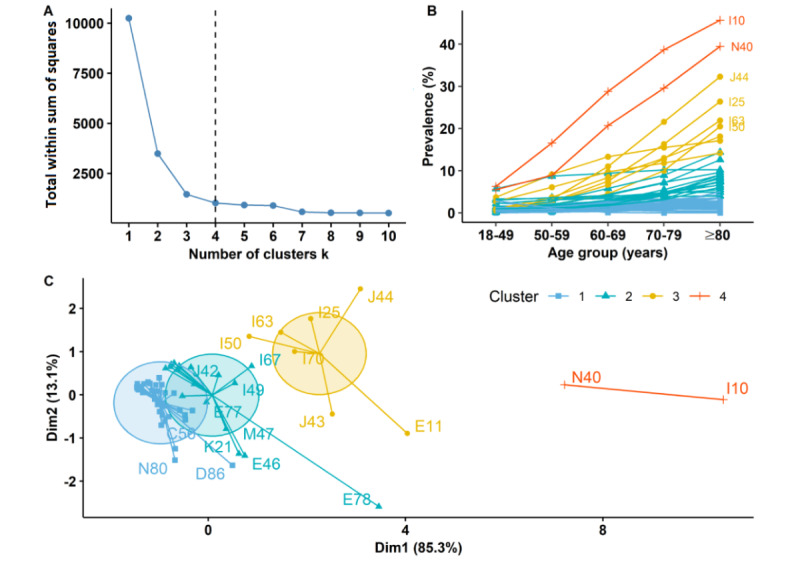
Results: A total of 29,610 new CRC cases occurred in Sichuan, China in 2020. The mean patient age at diagnosis was 65.6 (SD 12.9) years, and 75.5% (22,369/29,610) had at least one comorbidity. The most prevalent comorbidities were hypertension (8581/29,610, 29.0%; 95% CI 28.5%-29.5%), hyperplasia of the prostate (3816/17,426, 21.9%; 95% CI 21.3%-22.5%), and chronic obstructive pulmonary disease (COPD; 4199/29,610, 14.2%; 95% CI 13.8%-14.6%). The prevalence of single comorbidities was different in each subgroup in most cases. Comorbidities were closely associated, with disorders of lipoprotein metabolism and hyperplasia of the prostate mediating correlations between other comorbidities. Males and females shared 58.3% (141/242) of disease pairs, whereas male-female disparities occurred primarily in diseases coexisting with COPD, cerebrovascular diseases, atherosclerosis, heart failure, or renal failure among males and with osteoporosis or gonarthrosis among females. Urban patients generally had more comorbidities with higher prevalence and more complex disease coexistence relationships, whereas rural patients were more likely to have co-existing severe diseases, such as heart failure comorbid with the sequelae of cerebrovascular disease or COPD.
Conclusions: Male-female and urban-rural disparities in the prevalence of single comorbidities and their complex coexistence relationships in new CRC cases were not due to simple coincidence. The results reflect clinical practice in CRC patients and emphasize the importance of measuring comorbidity patterns in terms of individual and coexisting diseases in order to better understand comorbidity patterns.
Keywords: colorectal cancer; comorbidity patterns; health status disparities; network analysis; prevalence; routinely collected health data.
©Hang Qiu, Liya Wang, Li Zhou, Xiaodong Wang. Originally published in JMIR Public Health and Surveillance (https://publichealth.jmir.org), 05.09.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May;71(3):209–249. doi: 10.3322/caac.21660. https://onlinelibrary.wiley.com/doi/10.3322/caac.21660 - DOI - PubMed
-
- Xi Y, Xu P. Global colorectal cancer burden in 2020 and projections to 2040. Transl Oncol. 2021 Oct;14(10):101174. doi: 10.1016/j.tranon.2021.101174. https://linkinghub.elsevier.com/retrieve/pii/S1936-5233(21)00166-2 S1936-5233(21)00166-2 - DOI - PMC - PubMed
-
- Li N, Lu B, Luo C, Cai J, Lu M, Zhang Y, Chen H, Dai M. Incidence, mortality, survival, risk factor and screening of colorectal cancer: A comparison among China, Europe, and northern America. Cancer Lett. 2021 Dec 01;522:255–268. doi: 10.1016/j.canlet.2021.09.034.S0304-3835(21)00495-X - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
