

Pathological pallidal beta activity in Parkinson's disease is sustained during sleep and associated with sleep disturbance
- PMID: 37669927
- PMCID: PMC10480217
- DOI: 10.1038/s41467-023-41128-6
Pathological pallidal beta activity in Parkinson's disease is sustained during sleep and associated with sleep disturbance
Abstract
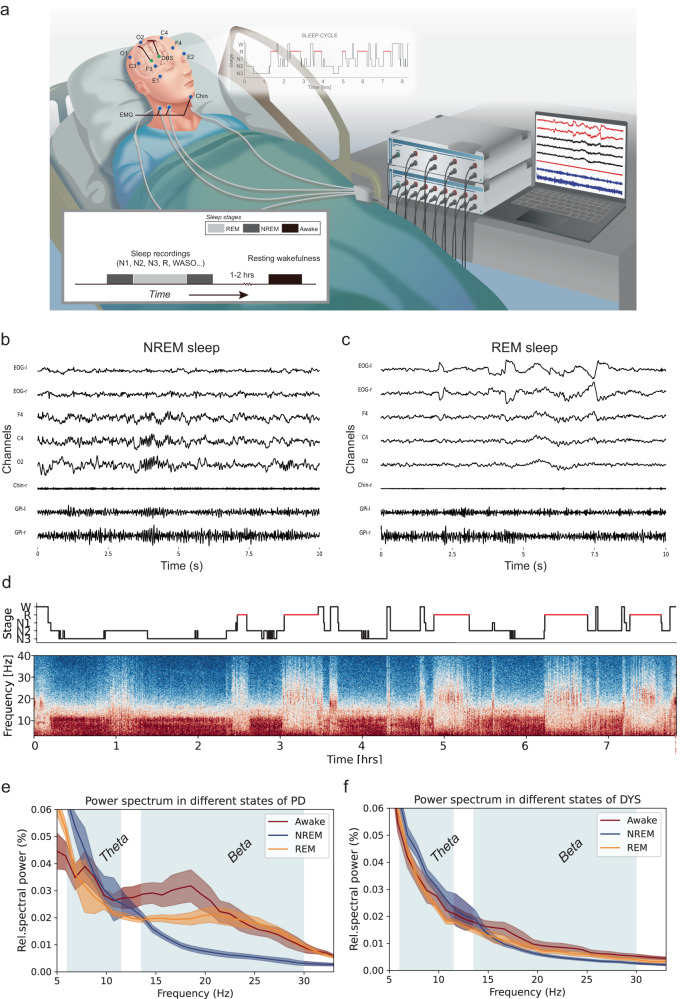
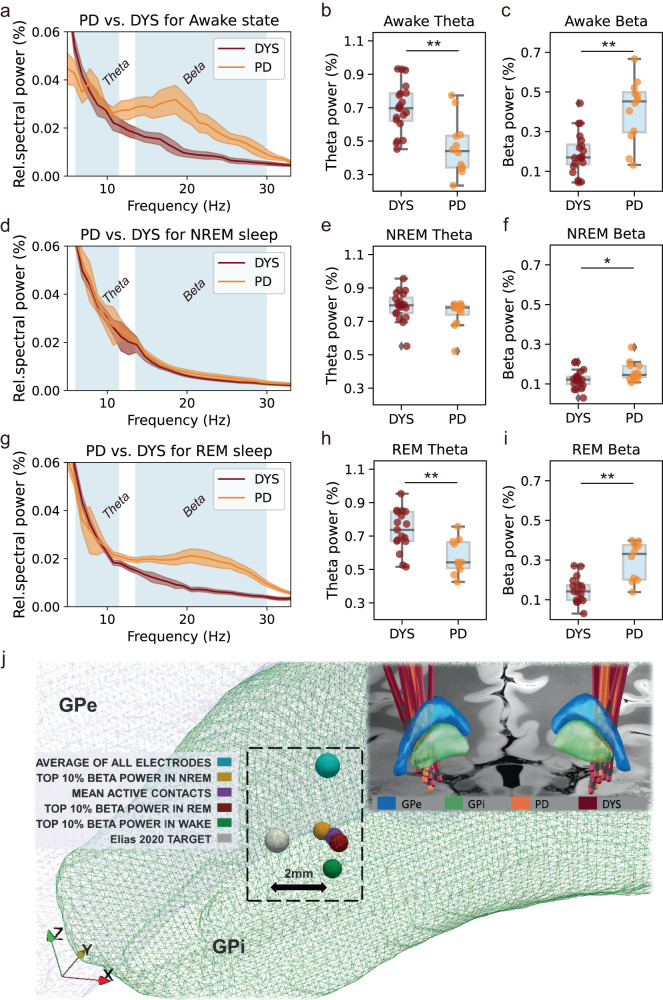
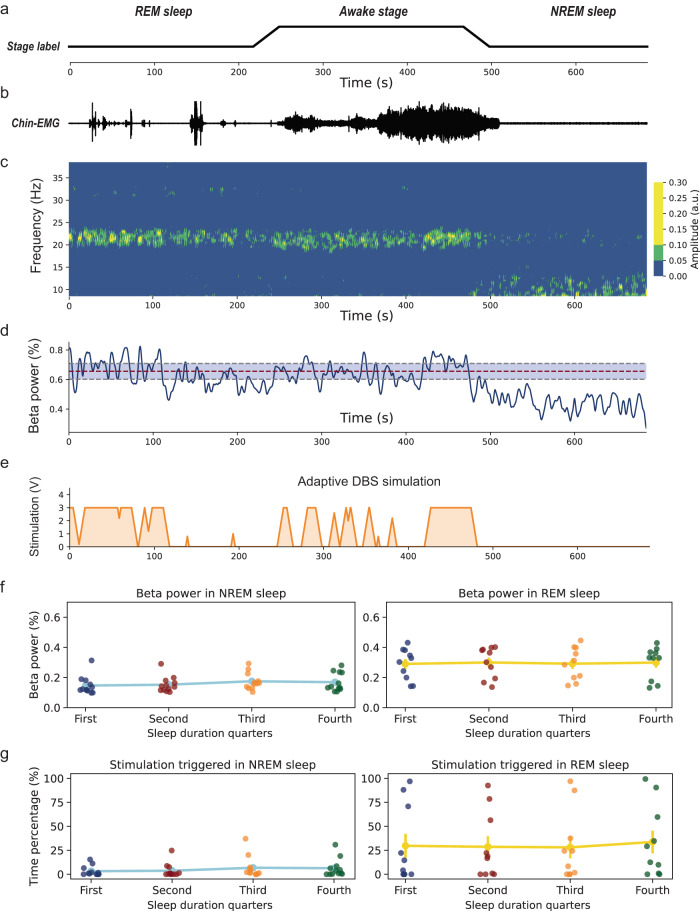
Parkinson's disease (PD) is associated with excessive beta activity in the basal ganglia. Brain sensing implants aim to leverage this biomarker for demand-dependent adaptive stimulation. Sleep disturbance is among the most common non-motor symptoms in PD, but its relationship with beta activity is unknown. To investigate the clinical potential of beta activity as a biomarker for sleep quality in PD, we recorded pallidal local field potentials during polysomnography in PD patients off dopaminergic medication and compared the results to dystonia patients. PD patients exhibited sustained and elevated beta activity across wakefulness, rapid eye movement (REM), and non-REM sleep, which was correlated with sleep disturbance. Simulation of adaptive stimulation revealed that sleep-related beta activity changes remain unaccounted for by current algorithms, with potential negative outcomes in sleep quality and overall quality of life for patients.
© 2023. Springer Nature Limited.
Conflict of interest statement
W.-J.N. received honoraria for talks unrelated to this manuscript from Medtronic which is a manufacturer of deep brain stimulation devices. A.A.K. is on the advisory board of Boston Scientific and Medtronic and has received honoraria unrelated to this manuscript from Boston Scientific, Medtronic, Stadapharm, and Teva, companies manufacturing deep brain stimulation or pharmaceutical therapies. H.B. is a consultant of Alpha Omega and has received travel honoraria from Boston Scientific and Medtronic unrelated to this manuscript. The remaining authors declare no competing interests.
Figures

References
-
- Zahed H, et al. The neurophysiology of sleep in Parkinson’s disease. Mov. Disord. 2021;36:1526–1542. - PubMed
-
- Garcia-Borreguero D, Larrosa O, Bravo M. Parkinson’s disease and sleep. Sleep Med. Rev. 2003;7:115–129. - PubMed
-
- Postuma RB, Gagnon JF, Vendette M, Charland K, Montplaisir J. REM sleep behaviour disorder in Parkinson’s disease is associated with specific motor features. J. Neurol. Neurosurg. Psychiatry. 2008;79:1117–1121. - PubMed
-
- Postuma RB, Gagnon J-F, Vendette M, Charland K, Montplaisir J. Manifestations of Parkinson disease differ in association with REM sleep behavior disorder. Mov. Disord. 2008;23:1665–1672. - PubMed
-
- Vendette M, et al. REM sleep behavior disorder predicts cognitive impairment in Parkinson disease without dementia. Neurology. 2007;69:1843–1849. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
