

Distinct smell and taste disorder phenotype of post-acute COVID-19 sequelae
- PMID: 37670171
- PMCID: PMC10562286
- DOI: 10.1007/s00405-023-08163-x
Distinct smell and taste disorder phenotype of post-acute COVID-19 sequelae
Abstract
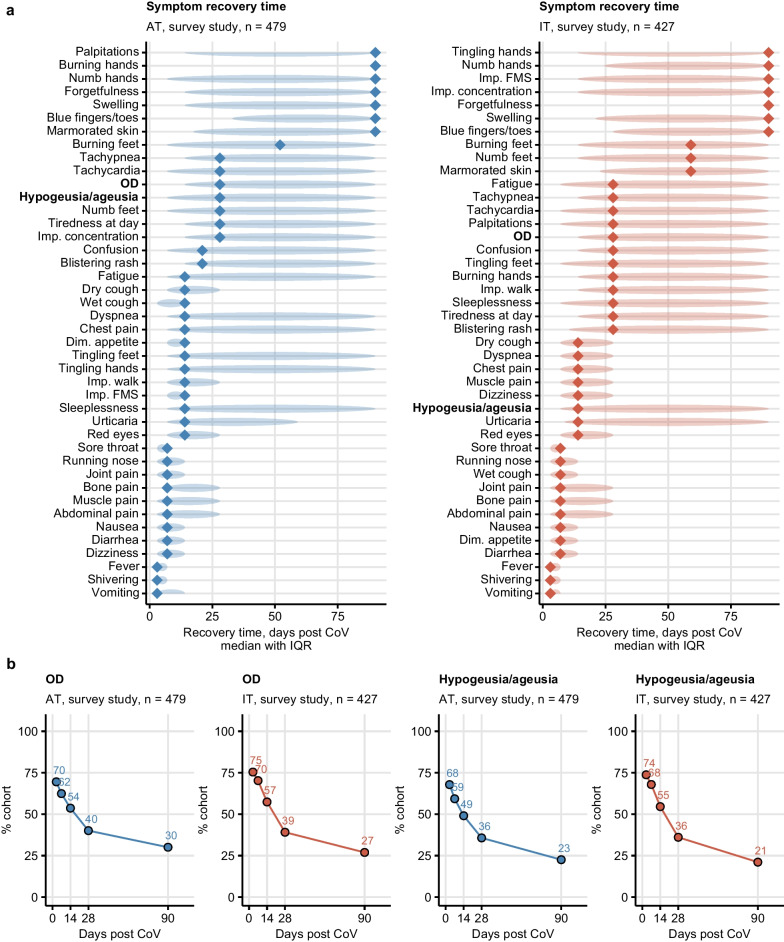
Purpose: Olfactory dysfunction (OD) commonly accompanies coronavirus disease 2019 (COVID-19). We investigated the kinetics of OD resolution following SARS-CoV-2 infection (wild-type and alpha variant) and its impact on quality of life, physical and mental health.
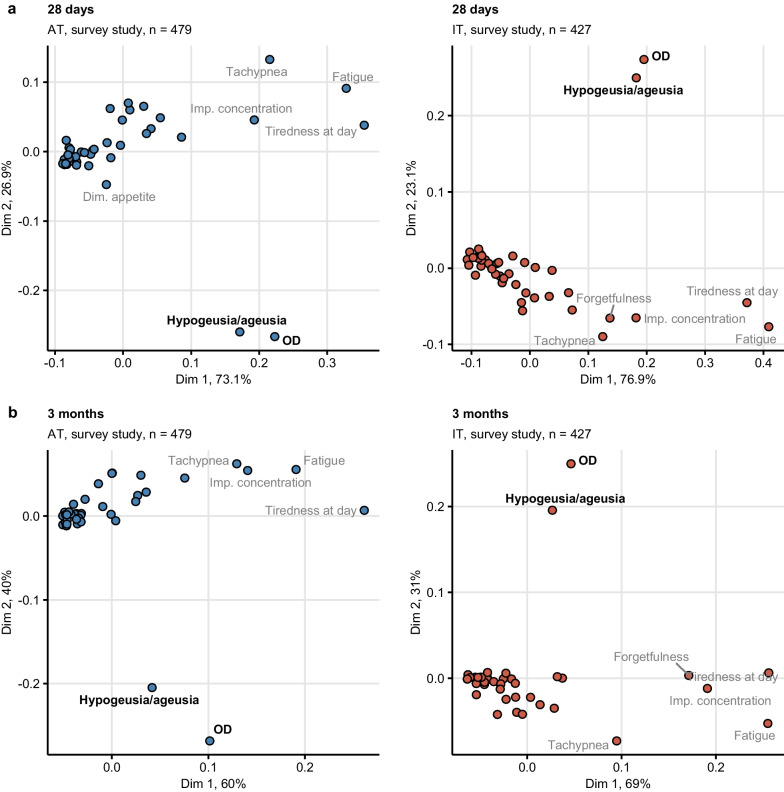
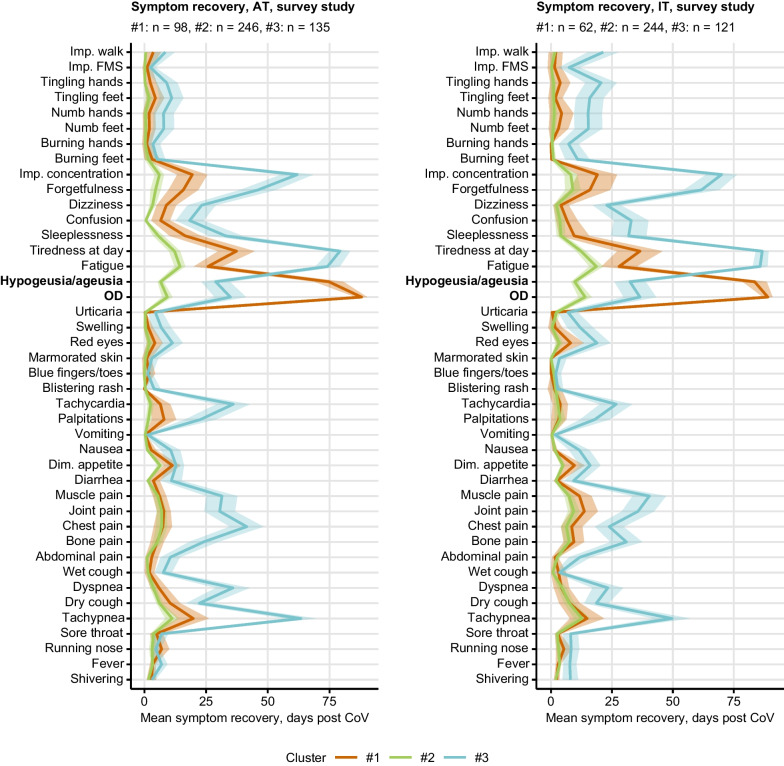
Methods: OD prevalence was assessed in an ambulatory COVID-19 survey (n = 906, ≥ 90 days follow-up) and an observational cohort of ambulatory and hospitalized individuals (n = 108, 360 days follow-up). Co-occurrence of OD with other symptoms and effects on quality of life, physical and mental health were analyzed by multi-dimensional scaling, association rule mining and semi-supervised clustering.
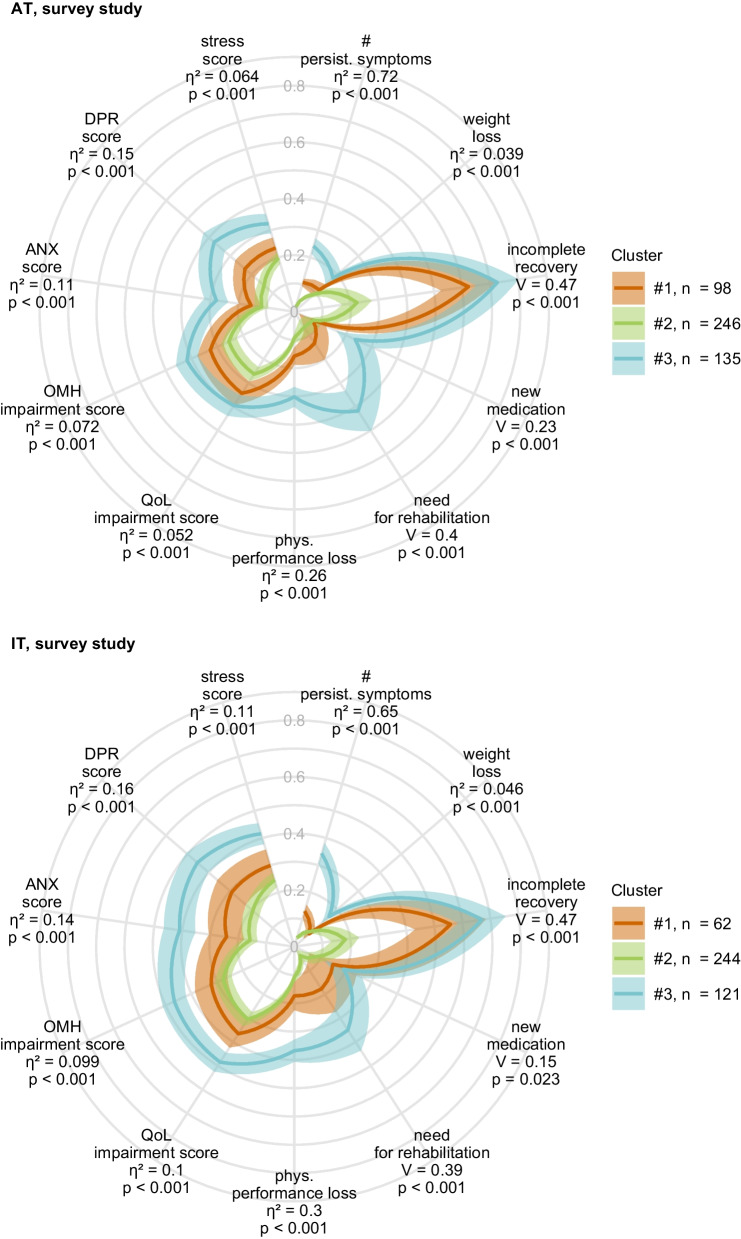
Results: Both in the ambulatory COVID-19 survey study (72%) and the observational ambulatory and hospitalized cohort (41%) self-reported OD was frequent during acute COVID-19. Recovery from self-reported OD was slow (survey: median 28 days, observational cohort: 90 days). By clustering of the survey data, we identified a predominantly young, female, comorbidity-free group of convalescents with persistent OD and taste disorders (median recovery: 90 days) but low frequency of post-acute fatigue, respiratory or neurocognitive symptoms. This smell and taste disorder cluster was characterized by a high rating of physical performance, mental health, and quality of life as compared with convalescents affected by prolonged fatigue or neurocognitive complaints.
Conclusion: Our results underline the heterogeneity of post-acute COVID-19 sequelae calling for tailored management strategies. The persistent smell and taste disorder phenotype is characterized by good clinical, physical, and mental recovery and may pose a minor challenge for public health.
Study registration: ClinicalTrials.gov: NCT04661462 (survey study), NCT04416100 (observational cohort).
Keywords: Long COVID; Mental health; Olfactory dysfunction; Post-COVID-19 condition; Quality of life; Smell and taste disorder.
© 2023. The Author(s).
Conflict of interest statement
No support from any organization for the submitted work; PT owns a data science enterprise, Data Analytics as a Service Tirol, and has received an honorarium for statistical data analysis and scientific writing of the manuscript; no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
Publication types
MeSH terms
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
