

Regulatory T cell frequency in peripheral blood of women with advanced cervical Cancer including women living with HIV
- PMID: 37670247
- PMCID: PMC10481519
- DOI: 10.1186/s12885-023-11345-9
Regulatory T cell frequency in peripheral blood of women with advanced cervical Cancer including women living with HIV
Abstract
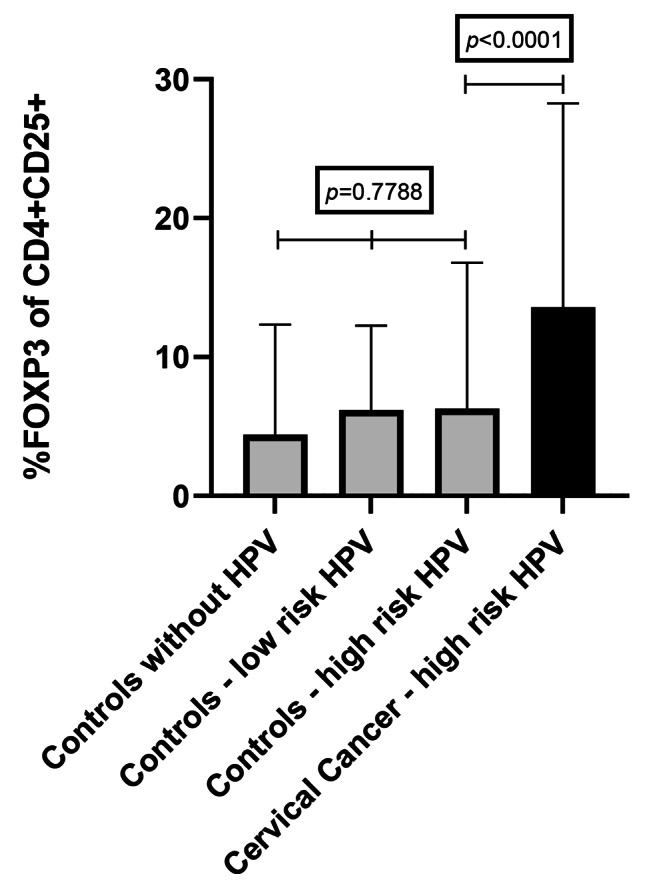
Background: Persistent high-risk Human papillomavirus (HR-HPV) infections are the main cause of cervical cancer. Cumulative evidence implicates regulatory T cells (Tregs) as a critical factor in the failure to eliminate HPV-induced cancers leading to their persistence and progression to cancer. Also, the WHO recognised cervical cancer as 100% attributable to persistent HR-HPV infection. The province of KwaZulu-Natal (KZN) in South Africa has a high prevalence of cervical cancer and HIV infection.
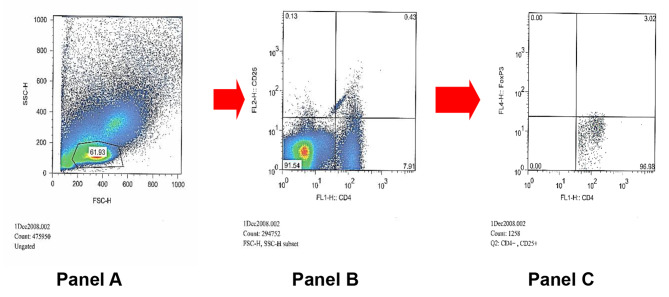
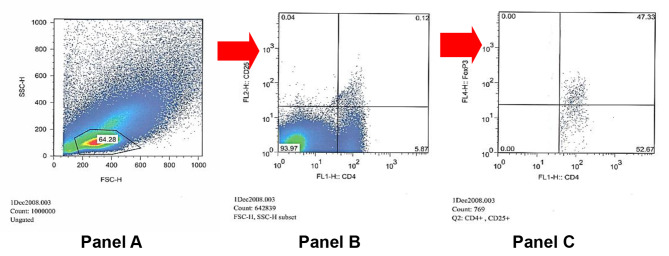
Materials and methods: We evaluated Treg frequency in dual infection of HR HPV and HIV coinfection using phenotypic markers, CD4, CD25 and intracellular Foxp3, in the peripheral blood of 51 cervical cancer and 46 non-cervical cancer participants and evaluated the effect of HIV on regulatory T cell proportion. Peripheral blood mononuclear cells were surface stained with a cocktail fluorescent labelled CD4 and CD25 and subsequently with APC anti-human FoxP3 (eBioscience). Flow cytometry was performed with FACS analysis. Statistical analysis of results was done using Instat 3 program (GraphpadR). Tregs results were expressed as median ± interquartile range (IQR). Associations of cervical cancer with demographic, clinical and laboratory variables were evaluated by univariate and multivariate logistic regression analysis using SPSS version 27 (IBM).
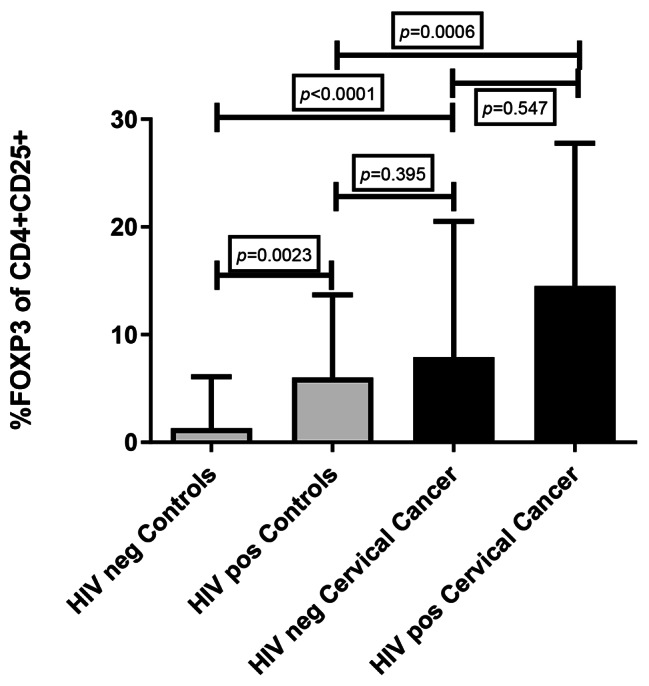
Results: Tregs frequency was significantly higher in individuals with cervical cancer (11.00 ± 19.79%) compared to controls (1.71 ± 8.91%) (p < 0.0001). HIV infection was associated with an increase in Tregs frequency. In controls a significant difference in Tregs frequency was noted between women living with HIV (6.00 ± 10.57%, n = 9) and those without HIV (1.30 ± 6.10%, n = 37), p = 0.0023. In multivariate logistic regression, Tregs frequency was significantly associated with cervical cancer after controlling for age, smoking, weight loss, presence of STI, HIV and HPV genotype.
Discussion/conclusion: Higher Tregs frequency was significantly associated with cervical cancer highlighting the immunosuppressive role of Tregs in cervical cancer. Treg frequency was more strongly associated with cervical cancer than HIV infection. We provide baseline data for monitoring Treg frequencies in response to new preventive and therapeutic strategies in the management of cervical cancer.
Keywords: Cervical cancer; HIV; Human papillomavirus; Immunosuppression; Regulatory T cells.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidences and mortality worldwide for 36 cancers in 185 countries.CA. Cancer J Clin. 2021;71209–49. 10.3322/caac.21660. - PubMed
-
- Stelzie D, Tanaka LF, Lee KK et al. Estimation of the global burden of cervical cancer associated with HIV. Lancet Glob Health 2020; published online Nov 16. DOI: S2214-109x(20)30459-9.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
