

Intra-operative applications of augmented reality in glioma surgery: a systematic review
- PMID: 37671031
- PMCID: PMC10476869
- DOI: 10.3389/fsurg.2023.1245851
Intra-operative applications of augmented reality in glioma surgery: a systematic review
Abstract
Background: Augmented reality (AR) is increasingly being explored in neurosurgical practice. By visualizing patient-specific, three-dimensional (3D) models in real time, surgeons can improve their spatial understanding of complex anatomy and pathology, thereby optimizing intra-operative navigation, localization, and resection. Here, we aimed to capture applications of AR in glioma surgery, their current status and future potential.
Methods: A systematic review of the literature was conducted. This adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. PubMed, Embase, and Scopus electronic databases were queried from inception to October 10, 2022. Leveraging the Population, Intervention, Comparison, Outcomes, and Study design (PICOS) framework, study eligibility was evaluated in the qualitative synthesis. Data regarding AR workflow, surgical application, and associated outcomes were then extracted. The quality of evidence was additionally examined, using hierarchical classes of evidence in neurosurgery.
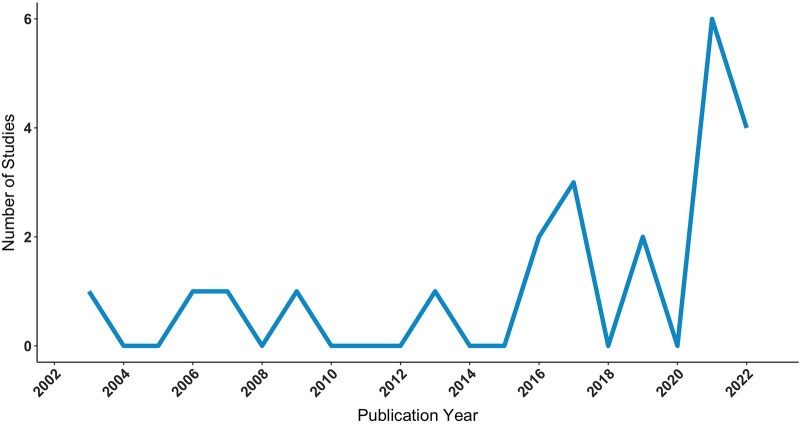
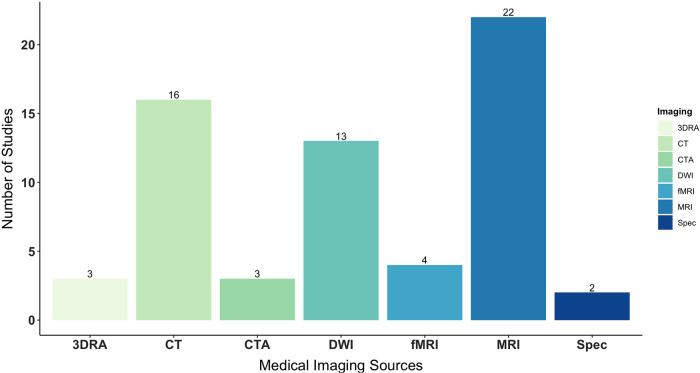
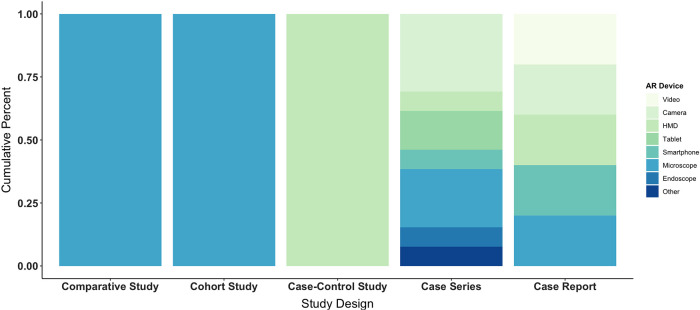
Results: The search returned 77 articles. Forty were subject to title and abstract screening, while 25 proceeded to full text screening. Of these, 22 articles met eligibility criteria and were included in the final review. During abstraction, studies were classified as "development" or "intervention" based on primary aims. Overall, AR was qualitatively advantageous, due to enhanced visualization of gliomas and critical structures, frequently aiding in maximal safe resection. Non-rigid applications were also useful in disclosing and compensating for intra-operative brain shift. Irrespective, there was high variance in registration methods and measurements, which considerably impacted projection accuracy. Most studies were of low-level evidence, yielding heterogeneous results.
Conclusions: AR has increasing potential for glioma surgery, with capacity to positively influence the onco-functional balance. However, technical and design limitations are readily apparent. The field must consider the importance of consistency and replicability, as well as the level of evidence, to effectively converge on standard approaches that maximize patient benefit.
Keywords: augmented reality; brain tumor; glioma; mixed reality; neuronavigation; neurosurgery; systematic review; virtual reality.
© 2023 Ragnhildstveit, Li, Zimmerman, Mamalakis, Curry, Holle, Baig, Uğuralp, Alkhani, Oğuz-Uğuralp, Romero-Garcia and Suckling.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- American Association of Neurological Surgeon. Brain Tumors. Available at: https://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments... (Accessed August 19, 2021).
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous