

Racial Disparities in Obesity-Related Cardiovascular Mortality in the United States: Temporal Trends From 1999 to 2020
- PMID: 37671611
- PMCID: PMC10547286
- DOI: 10.1161/JAHA.122.028409
Racial Disparities in Obesity-Related Cardiovascular Mortality in the United States: Temporal Trends From 1999 to 2020
Abstract
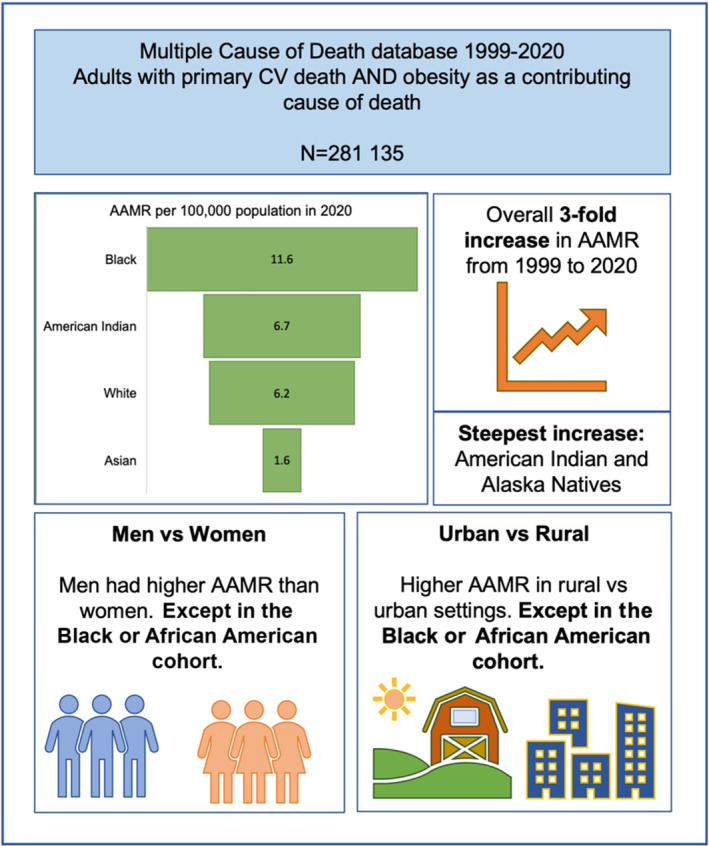
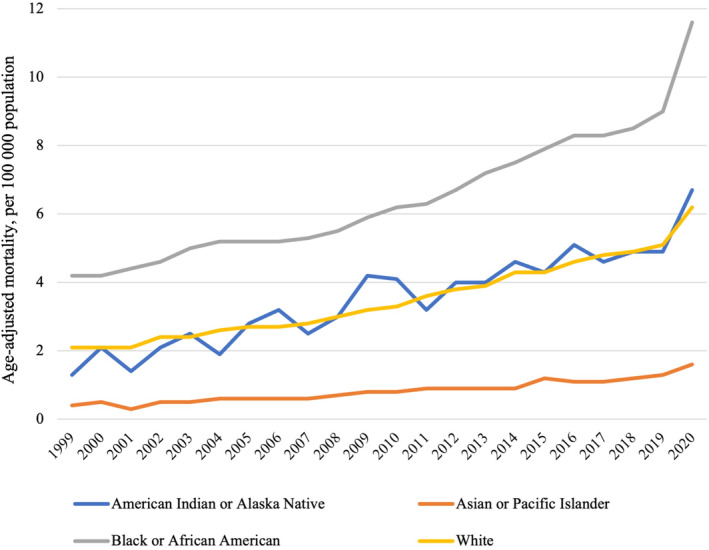
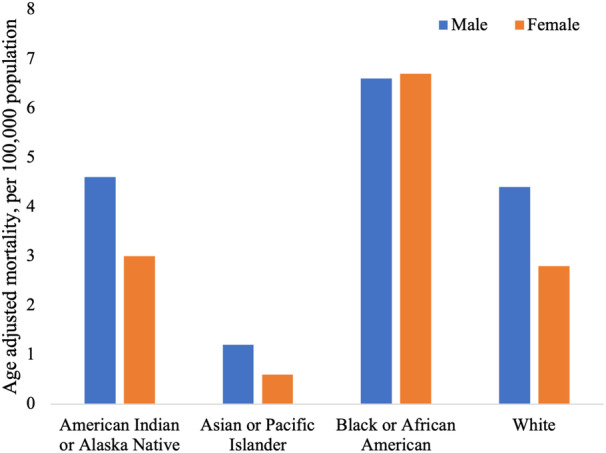
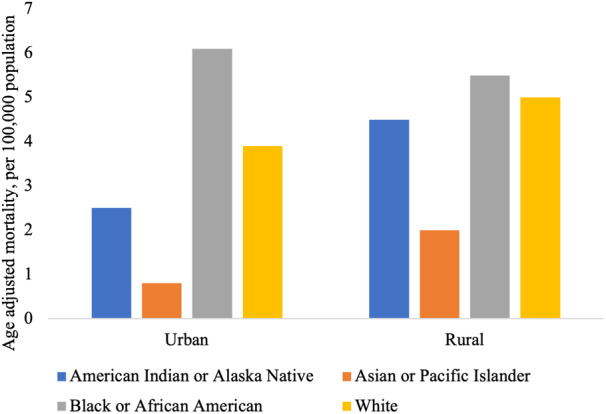
Background Obesity is a major risk factor for cardiovascular disease, with differential impact across populations. This descriptive epidemiologic study outlines trends and disparities in obesity-related cardiovascular mortality in the US population between 1999 and 2020. Methods and Results The Multiple Cause of Death database was used to identify adults with primary cardiovascular death and obesity recorded as a contributing cause of death. Cardiovascular deaths were grouped into ischemic heart disease, heart failure, hypertensive disease, cerebrovascular disease, and other. Absolute, crude, and age-adjusted mortality rates (AAMRs) were calculated by racial group, considering temporal trends and variation by sex, age, and residence (urban versus rural). Analysis of 281 135 obesity-related cardiovascular deaths demonstrated a 3-fold increase in AAMRs from 1999 to 2020 (2.2-6.6 per 100 000 population). Black individuals had the highest AAMRs. American Indian or Alaska Native individuals had the greatest temporal increase in AAMRs (+415%). Ischemic heart disease was the most common primary cause of death. The second most common cause of death was hypertensive disease, which was most common in the Black racial group (31%). Among Black individuals, women had higher AAMRs than men; across all other racial groups, men had a greater proportion of obesity-related cardiovascular mortality cases and higher AAMRs. Black individuals had greater AAMRs in urban compared with rural settings; the reverse was observed for all other races. Conclusions Obesity-related cardiovascular mortality is increasing with differential trends by race, sex, and place of residence.
Keywords: body mass index; cardiovascular disease; epidemiology; ethnicity; health inequalities; public health.
Figures

References
-
- Stierman B, Afful J, Carroll MD, Te‐Ching C, Orlando D, Fink S, Fryar CD, Gu Q, Hales CM, Hughes JP, et al. National Health and Nutrition Examination Survey 2017–March 2020. Prepandemic data files development of files and prevalence estimates for selected health outcomes. 2021. National Health Statistics Reports. Accessed August 2, 2023. https://stacks.cdc.gov/view/cdc/106273.
-
- Bentham J, Di Cesare M, Bilano V, Bixby H, Zhou B, Stevens GA, Riley LM, Taddei C, Hajifathalian K, Lu Y, et al. Worldwide trends in body‐mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population‐based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390:2627–2642. doi: 10.1016/S0140-6736(17)32129-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
