

Intensive Statin Therapy Versus Upfront Combination Therapy of Statin and Ezetimibe in Patients With Acute Coronary Syndrome: A Propensity Score Matching Analysis Based on the PL-ACS Data
- PMID: 37671618
- PMCID: PMC10547305
- DOI: 10.1161/JAHA.123.030414
Intensive Statin Therapy Versus Upfront Combination Therapy of Statin and Ezetimibe in Patients With Acute Coronary Syndrome: A Propensity Score Matching Analysis Based on the PL-ACS Data
Abstract
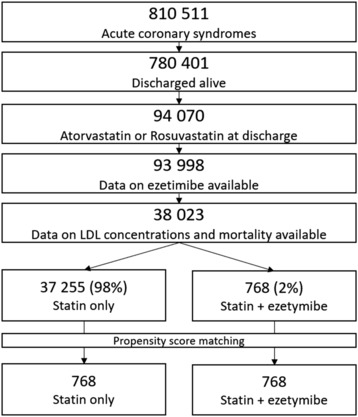
Background We aimed to compare statin monotherapy and upfront combination therapy of statin and ezetimibe in patients with acute coronary syndromes (ACSs). Methods and Results The study included consecutive patients with ACS included in the PL-ACS (Polish Registry of Acute Coronary Syndromes), which is a national, multicenter, ongoing, prospective observational registry that is mandatory for patients with ACS hospitalized in Poland. Data were matched using the Mahalanobis distance within propensity score matching calipers. Multivariable stepwise logistic regression analysis, including all variables, was next used in propensity score matching analysis. Finally, 38 023 consecutive patients with ACS who were discharged alive were included in the analysis. After propensity score matching, 2 groups were analyzed: statin monotherapy (atorvastatin or rosuvastatin; n=768) and upfront combination therapy of statin and ezetimibe (n=768 patients). The difference in mortality between groups was significant during the follow-up and was present at 1 (5.9% versus 3.5%; P=0.041), 2 (7.8% versus 4.3%; P=0.019), and 3 (10.2% versus 5.5%; P=0.024) years of follow-up in favor of the upfront combination therapy, as well as for the overall period. For the treatment, rosuvastatin significantly improved prognosis compared with atorvastatin (odds ratio [OR], 0.790 [95% CI, 0.732-0.853]). Upfront combination therapy was associated with a significant reduction of all-cause mortality in comparison with statin monotherapy (OR, 0.526 [95% CI, 0.378-0.733]), with absolute risk reduction of 4.7% after 3 years (number needed to treat=21). Conclusions The upfront combination lipid-lowering therapy is superior to statin monotherapy for all-cause mortality in patients with ACS. These results suggest that in high-risk patients, such an approach, rather than a stepwise therapy approach, should be recommended.
Keywords: acute coronary syndrome; combination therapy; lipids; monotherapy; prevention.
Figures

Comment in
-
Upfront Combination of Statin and Ezetimibe for Patients With Acute Coronary Syndrome: Time for a New Approach?J Am Heart Assoc. 2023 Sep 19;12(18):e031615. doi: 10.1161/JAHA.123.031615. Epub 2023 Sep 6. J Am Heart Assoc. 2023. PMID: 37671619 Free PMC article. No abstract available.
References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010 - DOI - PMC - PubMed
-
- Ference BA, Ginsberg HN, Graham I, Ray KK, Packard CJ, Bruckert E, Hegele RA, Krauss RM, Raal FJ, Schunkert H, et al. Low‐density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38:2459–2472. doi: 10.1093/eurheartj/ehx144 - DOI - PMC - PubMed
-
- Ray KK, Molemans B, Schoonen WM, Giovas P, Bray S, Kiru G, Murphy J, Banach M, De Servi S, Gaita D, et al. EU‐wide cross‐sectional observational study of lipid‐modifying therapy use in secondary and primary care: the DA VINCI study. Eur J Prev Cardiol. 2021;28:1279–1289. doi: 10.1093/eurjpc/zwaa047 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
