

Response to glecaprevir/pibrentasvir in HIV/HCV-coinfected patients in clinical practice
- PMID: 37671831
- PMCID: PMC10775154
- DOI: 10.1093/jac/dkad278
Response to glecaprevir/pibrentasvir in HIV/HCV-coinfected patients in clinical practice
Abstract
Objectives: HIV infection has been associated with lower rates of sustained viral response (SVR) with direct-acting antivirals (DAAs). There are few data on glecaprevir/pibrentasvir (G/P) in HIV/HCV coinfection outside clinical trials.
Methods: The HEPAVIR-DAA cohort, which recruits HIV/HCV-coinfected patients (NCT02057003) and the GEHEP-MONO cohort (NCT02333292), including HCV-monoinfected individuals, are two concurrent ongoing multicentre cohorts of patients receiving anti-HCV treatment. Patients starting G/P included in those cohorts were analysed. Overall SVR (ITT), discontinuations due to adverse effects, and dropouts were evaluated and compared between both cohorts.
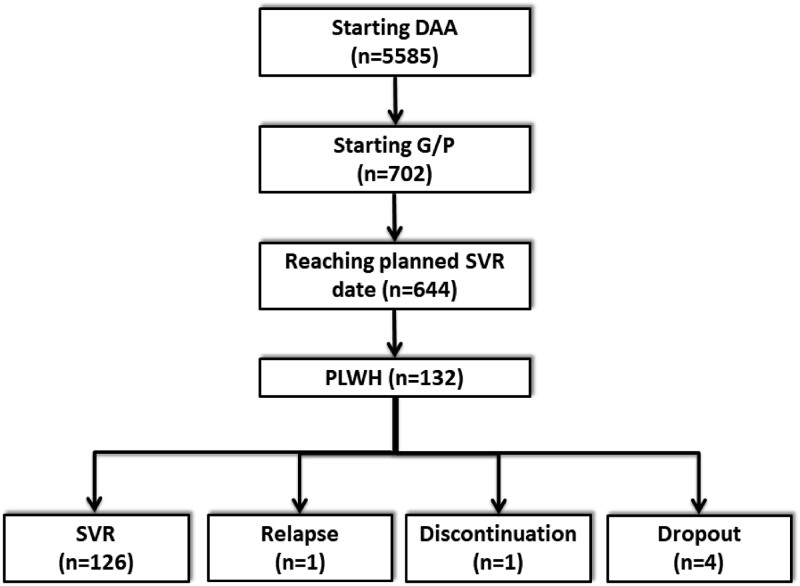
Results: Of the 644 patients who started G/P with evaluable SVR, 132 were HIV/HCV coinfected. Overall SVR rates were 487/512 (95.1%) in HCV-monoinfected patients versus 126/132 (95.5%) in HIV/HCV-coinfected patients (P = 1.000). One patient (0.8%) relapsed, and another (0.8%) discontinued treatment due to side effects. SVR to 8 or 12 weeks of treatment with G/P was similar in HIV/HCV-coinfected versus HCV-monoinfected patients. The main reason for not reaching SVR among HIV/HCV-coinfected patients was premature dropout linked to active drug use.
Conclusions: G/P in HIV/HCV coinfection was highly effective and tolerable in clinical practice. SVR to 8 or 12 weeks of treatment with G/P was similar in HIV/HCV-coinfected compared with HCV-monoinfected patients but active drug use is still a barrier to reach HCV microelimination.
© The Author(s) 2023. Published by Oxford University Press on behalf of British Society for Antimicrobial Chemotherapy. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
References
-
- Forns X, Lee SS, Valdes J et al. Glecaprevir plus pibrentasvir for chronic hepatitis C virus genotype 1, 2, 4, 5, or 6 infection in adults with compensated cirrhosis (EXPEDITION-1): a single-arm, open-label, multicentre phase 3 trial. Lancet Infect Dis 2017; 17: 1062–8. 10.1016/S1473-3099(17)30496-6 - DOI - PubMed
