

Methodological and ethical challenges in the use of focused ultrasound for blood-brain barrier disruption in neuro-oncology
- PMID: 37672093
- PMCID: PMC10739192
- DOI: 10.1007/s00701-023-05782-5
Methodological and ethical challenges in the use of focused ultrasound for blood-brain barrier disruption in neuro-oncology
Abstract
Background: Focused ultrasound (FUS) shows promise for enhancing drug delivery to the brain by temporarily opening the blood-brain barrier (BBB), and it is increasingly used in the clinical setting to treat brain tumours. It remains however unclear whether FUS is being introduced in an ethically and methodologically sound manner. The IDEAL-D framework for the introduction of surgical innovations and the SYRCLE and ROBINS-I tools for assessing the risk of bias in animal studies and non-randomized trials, respectively, provide a comprehensive evaluation for this.
Objectives and methods: A comprehensive literature review on FUS in neuro-oncology was conducted. Subsequently, the included studies were evaluated using the IDEAL-D framework, SYRCLE, and ROBINS-I tools.
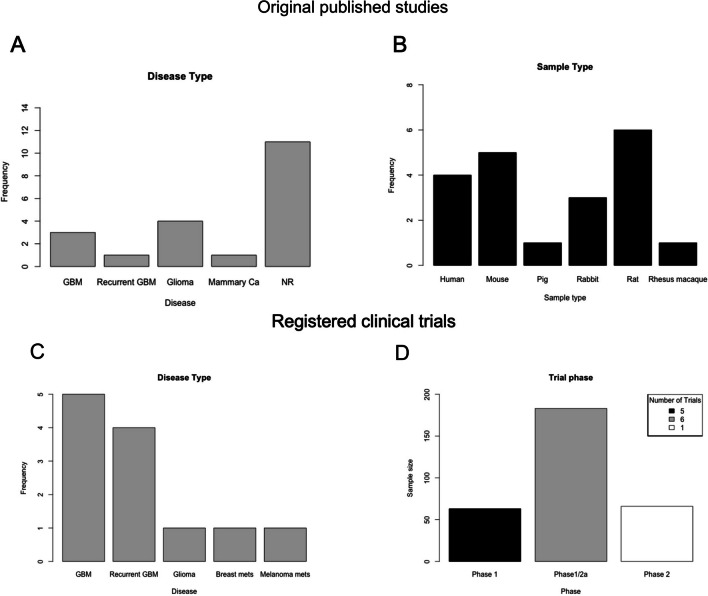
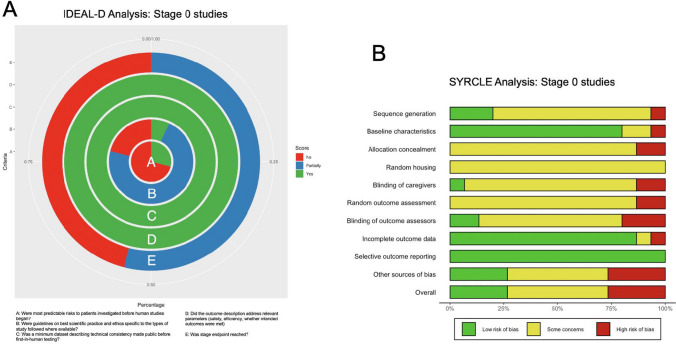
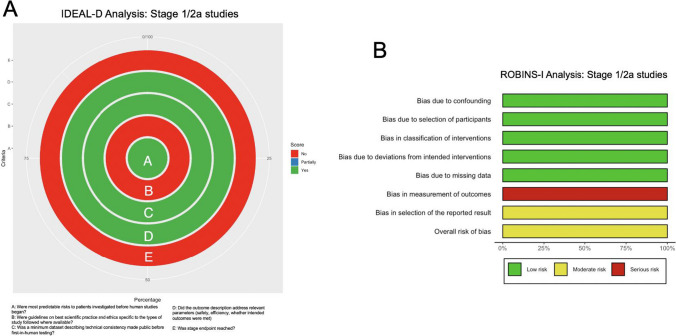
Results: In total, 19 published studies and 12 registered trials were identified. FUS demonstrated successful BBB disruption, increased drug delivery, and improved survival rates. However, the SYRCLE analysis revealed a high risk of bias in animal studies, while the ROBINS-I analysis found that most human studies had a high risk of bias due to a lack of blinding and heterogeneous samples. Of the 15 pre-clinical stage 0 studies, only six had formal ethical approval, and only five followed animal care policies. Both stage 1 studies and stage 1/2a studies failed to provide information on patient data confidentiality. Overall, no animal or human study reached the IDEAL-D stage endpoint.
Conclusion: FUS holds promise for enhancing drug delivery to the brain, but its development and implementation must adhere to rigorous safety standards using the established ethical and methodological frameworks. The complementary use of IDEAL-D, SYRCLE, and ROBINS-I tools indicates a high risk of bias and ethical limitations in both animal and human studies, highlighting the need for further improvements in study design for a safe implementation of FUS in neuro-oncology.
Keywords: Brain tumor; Focused ultrasound; Glioblastoma; Glioma; IDEAL; Neuro-oncology; ROBINS-I; SYRCLE.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Focused ultrasound blood-brain barrier disruption in high-grade gliomas: Scoping review of clinical studies.J Clin Neurosci. 2024 Oct;128:110786. doi: 10.1016/j.jocn.2024.110786. Epub 2024 Aug 14. J Clin Neurosci. 2024. PMID: 39146579
-
Translation of focused ultrasound for blood-brain barrier opening in glioma.J Control Release. 2022 May;345:443-463. doi: 10.1016/j.jconrel.2022.03.035. Epub 2022 Mar 23. J Control Release. 2022. PMID: 35337938 Review.
-
Focused Ultrasound-Mediated Blood-Brain Barrier Opening Increases Delivery and Efficacy of Etoposide for Glioblastoma Treatment.Int J Radiat Oncol Biol Phys. 2021 Jun 1;110(2):539-550. doi: 10.1016/j.ijrobp.2020.12.019. Epub 2020 Dec 17. Int J Radiat Oncol Biol Phys. 2021. PMID: 33346092 Free PMC article.
-
From Focused Ultrasound Tumor Ablation to Brain Blood Barrier Opening for High Grade Glioma: A Systematic Review.Cancers (Basel). 2021 Nov 10;13(22):5614. doi: 10.3390/cancers13225614. Cancers (Basel). 2021. PMID: 34830769 Free PMC article. Review.
-
Emerging Applications of Therapeutic Ultrasound in Neuro-oncology: Moving Beyond Tumor Ablation.Neurosurgery. 2016 Nov;79(5):643-654. doi: 10.1227/NEU.0000000000001399. Neurosurgery. 2016. PMID: 27552589 Free PMC article. Review.
Cited by
-
Focused ultrasound as a treatment modality for gliomas.Front Neurol. 2024 May 15;15:1387986. doi: 10.3389/fneur.2024.1387986. eCollection 2024. Front Neurol. 2024. PMID: 38813245 Free PMC article. Review.
-
Leptomeningeal metastatic disease: new frontiers and future directions.Nat Rev Clin Oncol. 2025 Feb;22(2):134-154. doi: 10.1038/s41571-024-00970-3. Epub 2024 Dec 9. Nat Rev Clin Oncol. 2025. PMID: 39653782 Review.
References
-
- Carpentier A, Canney M, Vignot A et al (2016) Clinical trial of blood-brain barrier disruption by pulsed ultrasound. Sci Transl Med 8(343). 10.1126/SCITRANSLMED.AAF6086/SUPPL_FILE/8-343RE2_SM.PDF - PubMed
-
- Conti A, Kamimura HAS, Novell A, Duggento A, Toschi N (2020) Magnetic resonance methods for focused ultrasound-induced blood-brain barrier opening. Front Phys 8. 10.3389/fphy.2020.547674
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
