

Nonrelapse mortality after CAR T-cell therapy for large B-cell lymphoma: a LYSA study from the DESCAR-T registry
- PMID: 37672383
- PMCID: PMC10641092
- DOI: 10.1182/bloodadvances.2023010624
Nonrelapse mortality after CAR T-cell therapy for large B-cell lymphoma: a LYSA study from the DESCAR-T registry
Abstract
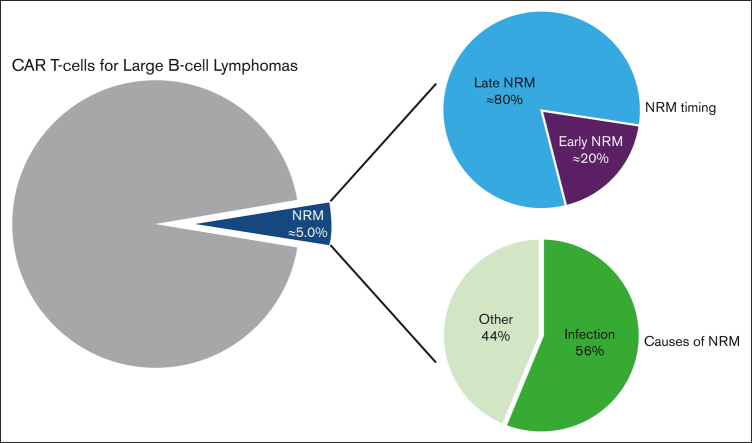
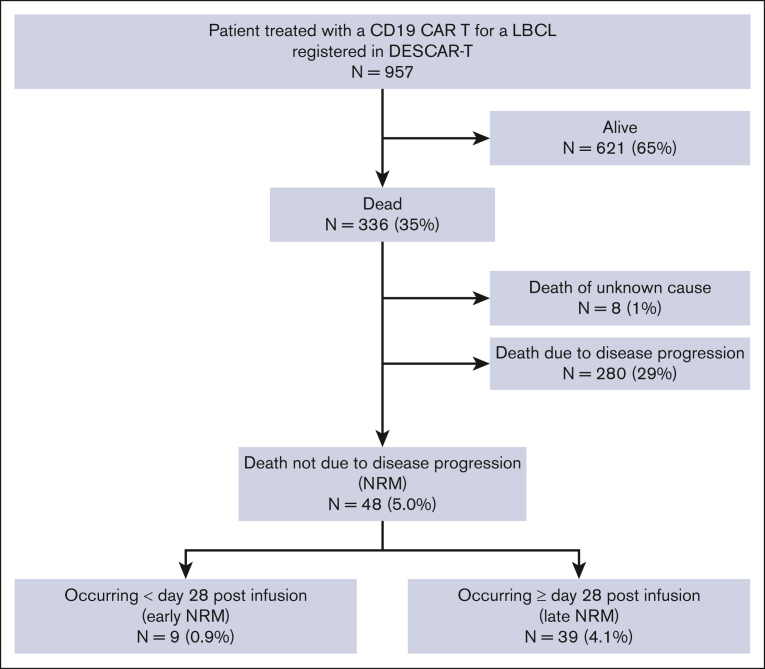
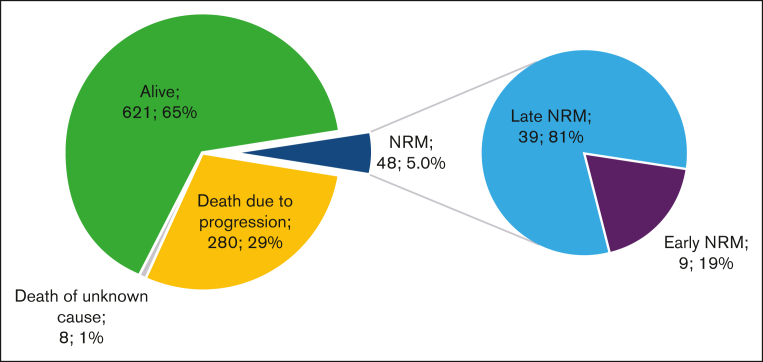
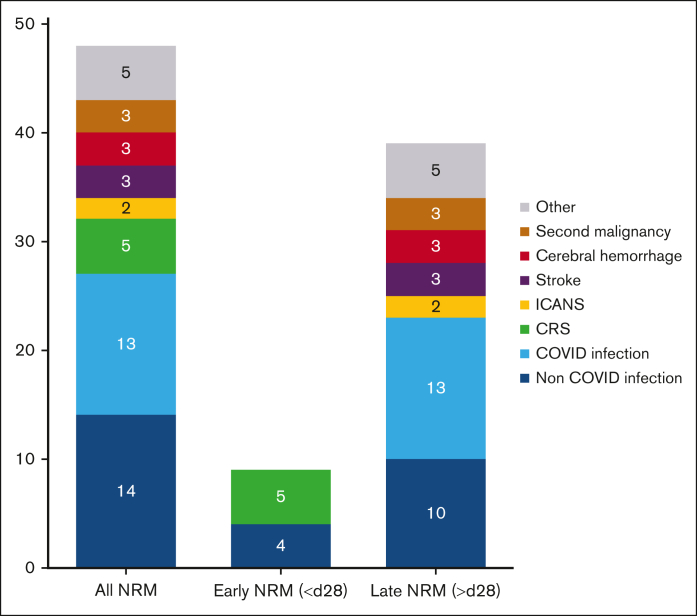
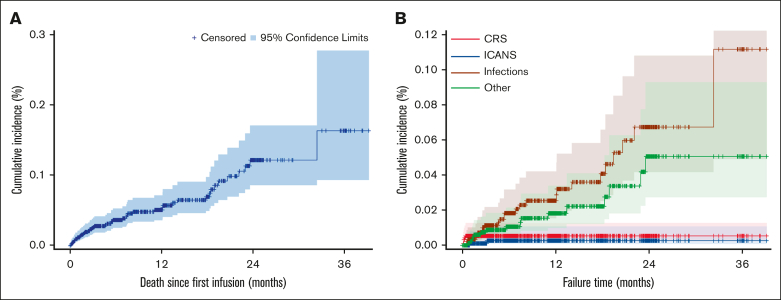
CD19 chimeric antigen receptor (CAR) T cells can induce prolonged remissions and potentially cure a significant proportion of patients with relapsed/refractory large B-cell lymphomas. However, some patients may die of causes unrelated to lymphoma after CAR T-cell therapy. To date, little is known about the nonrelapse mortality (NRM) after CAR T-cell therapy. Using the French DESCAR-T registry, we analyzed the incidence and causes of NRM and identified risk factors of NRM. We report on 957 patients who received standard-of-care axicabtagene ciloleucel (n = 598) or tisagenlecleucel (n = 359) between July 2018 and April 2022, in 27 French centers. With a median follow-up of 12.4 months, overall NRM occurred in 48 patients (5.0% of all patients): early (before day 28 after infusion) in 9 patients (0.9% of all patients and 19% of overall NRM), and late (on/after day 28 after infusion) in 39 patients (4.1% of all patients and 81% of overall NRM). Causes of overall NRM were distributed as follows: 56% infections (29% with non-COVID-19 and 27% with COVID-19), 10% cytokine release syndromes, 6% stroke, 6% cerebral hemorrhage, 6% second malignancies, 4% immune effector cell associated neurotoxicities, and 10% deaths from other causes. We report risk factors of early NRM and overall NRM. In multivariate analysis, both diabetes and elevated ferritin level at lymphodepletion were associated with an increased risk of overall NRM. Our results may help physicians in patient selection and management in order to reduce the NRM after CAR T-cell therapy.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: E.B. received honoraria from Kite, a Gilead Company, and Novartis. G.C. received honoraria from Kite, a Gilead Company, and Novartis. T.G. received honoraria from Kite, a Gilead Company. R.D.B. received honoraria from Kite, a Gilead Company, and Novartis. S.G. received honoraria from Kite/Gilead, Incyte, Takeda, and Janssen. M.M. received honoraria from Kite, a Gilead Company, and Novartis. R.-O.C. received honoraria from Kite, a Gilead Company. C.C.-L. received honoraria from Kite, a Gilead Company. M.L. received honoraria from Kite, a Gilead Company, and Novartis. S.L.G. reports consultancy for Kite, a Gilead Company, and Novartis. C.T. received honoraria from Kite, a Gilead Company, and Novartis. R.H. received honoraria from Kite, a Gilead Company, and Novartis. The remaining authors declare no competing financial interests.
Figures
References
-
- Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. 2019;380(1):45–56. - PubMed
-
- Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet Lond Engl. 2020;396(10254):839–852. - PubMed
-
- Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. N Engl J Med. 2022;386(7):640–654. - PubMed
-
- Kamdar M, Solomon SR, Arnason J, et al. Lisocabtagene maraleucel versus standard of care with salvage chemotherapy followed by autologous stem cell transplantation as second-line treatment in patients with relapsed or refractory large B-cell lymphoma (TRANSFORM): results from an interim analysis of an open-label, randomised, phase 3 trial. Lancet. 2022;399(10343):2294–2308. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
