

Atezolizumab for Advanced Alveolar Soft Part Sarcoma
- PMID: 37672694
- PMCID: PMC10729808
- DOI: 10.1056/NEJMoa2303383
Atezolizumab for Advanced Alveolar Soft Part Sarcoma
Abstract
Background: Alveolar soft part sarcoma (ASPS) is a rare soft-tissue sarcoma with a poor prognosis and no established therapy. Recently, encouraging responses to immune checkpoint inhibitors have been reported.
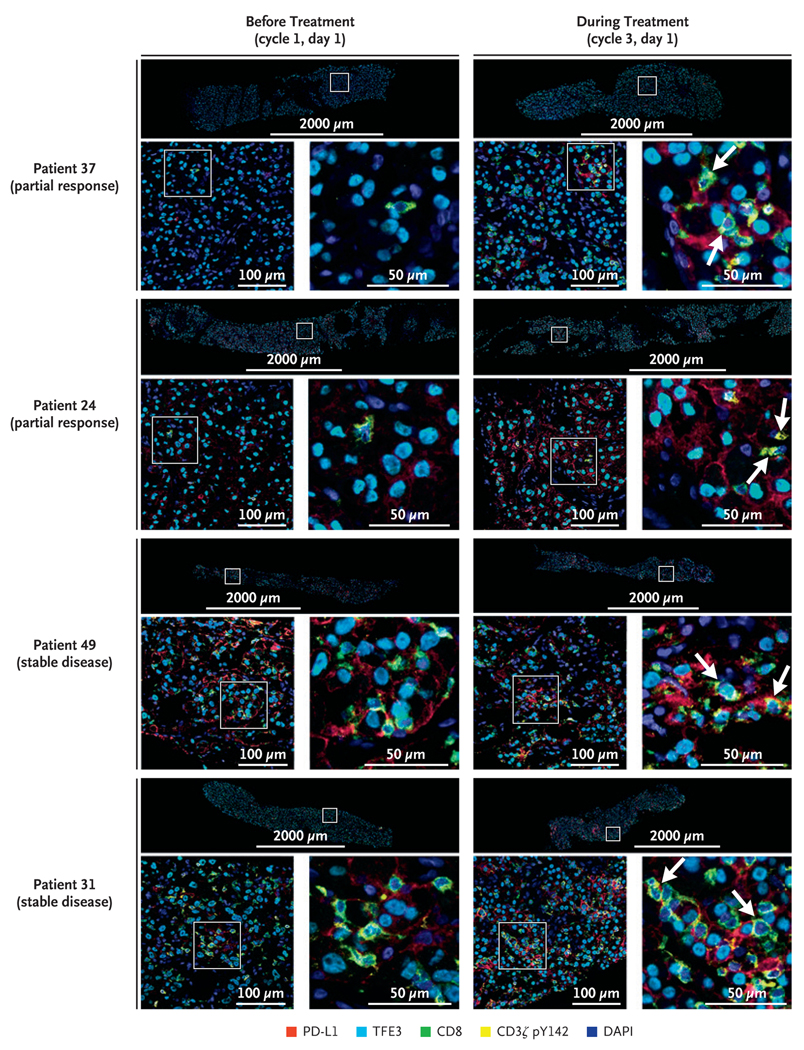
Methods: We conducted an investigator-initiated, multicenter, single-group, phase 2 study of the anti-programmed death ligand 1 (PD-L1) agent atezolizumab in adult and pediatric patients with advanced ASPS. Atezolizumab was administered intravenously at a dose of 1200 mg (in patients ≥18 years of age) or 15 mg per kilogram of body weight with a 1200-mg cap (in patients <18 years of age) once every 21 days. Study end points included objective response, duration of response, and progression-free survival according to Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1, as well as pharmacodynamic biomarkers of multistep drug action.
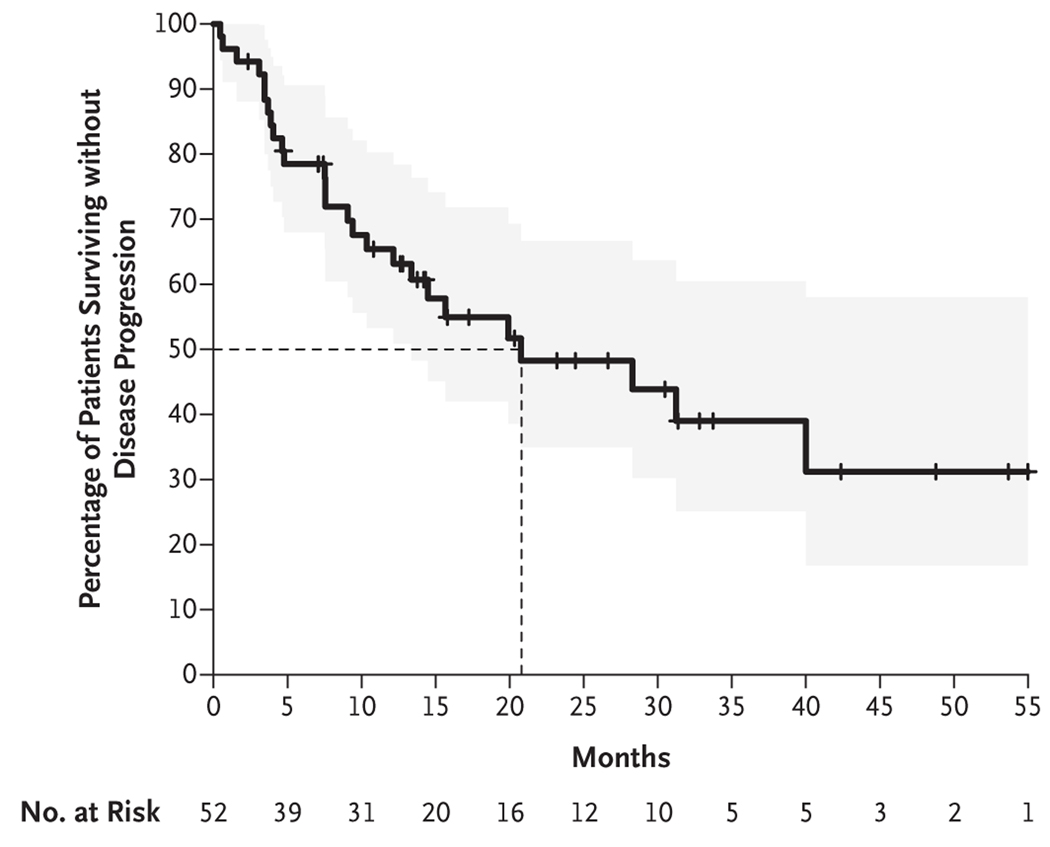
Results: A total of 52 patients were evaluated. An objective response was observed in 19 of 52 patients (37%), with 1 complete response and 18 partial responses. The median time to response was 3.6 months (range, 2.1 to 19.1), the median duration of response was 24.7 months (range, 4.1 to 55.8), and the median progression-free survival was 20.8 months. Seven patients took a treatment break after 2 years of treatment, and their responses were maintained through the data-cutoff date. No treatment-related grade 4 or 5 adverse events were recorded. Responses were noted despite variable baseline expression of programmed death 1 and PD-L1.
Conclusions: Atezolizumab was effective at inducing sustained responses in approximately one third of patients with advanced ASPS. (Funded by the National Cancer Institute and others; ClinicalTrials.gov number, NCT03141684.).
Copyright © 2023 Massachusetts Medical Society.
Figures


References
-
- O’Sullivan Coyne G, Naqash AR, Sankaran H, Chen AP. Advances in the management of alveolar soft part sarcoma. Curr Probl Cancer 2021; 45: 100775. - PubMed
-
- Ladanyi M, Lui MY, Antonescu CR, et al. The der(17)t(X;17)(p11;q25) of human alveolar soft part sarcoma fuses the TFE3 transcription factor gene to ASPL, a novel gene at 17q25. Oncogene 2001; 20: 48–57. - PubMed
-
- Williams A, Bartle G, Sumathi VP, et al. Detection of ASPL/TFE3 fusion transcripts and the TFE3 antigen in formalin-fixed, paraffin-embedded tissue in a series of 18 cases of alveolar soft part sarcoma: useful diagnostic tools in cases with unusual histological features. Virchows Arch 2011; 458: 291–300. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous