

Spatial predictors of immunotherapy response in triple-negative breast cancer
- PMID: 37674077
- PMCID: PMC10533410
- DOI: 10.1038/s41586-023-06498-3
Spatial predictors of immunotherapy response in triple-negative breast cancer
Abstract
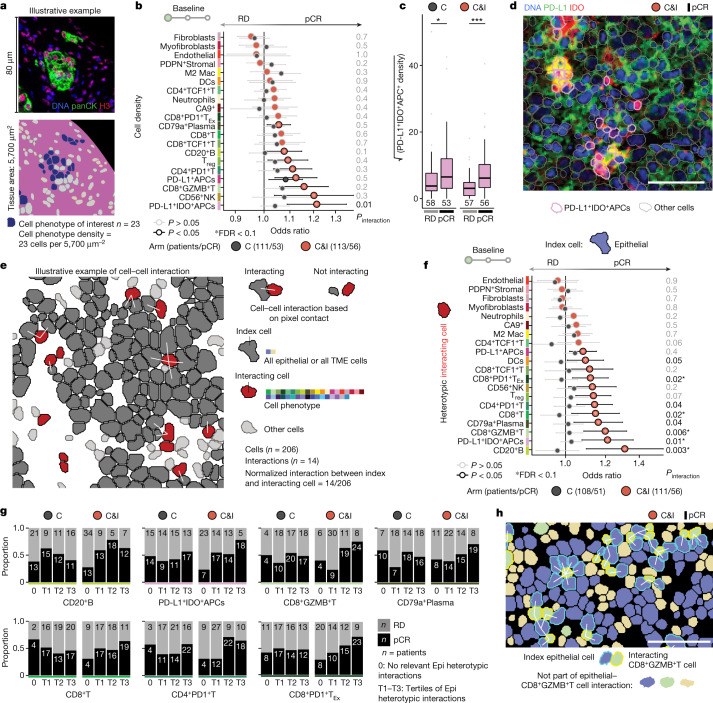
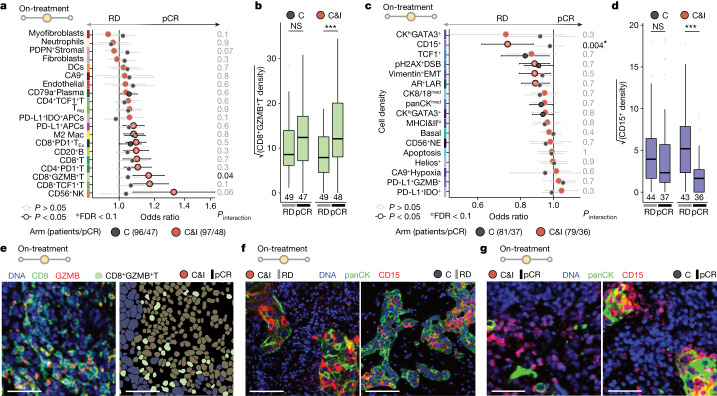
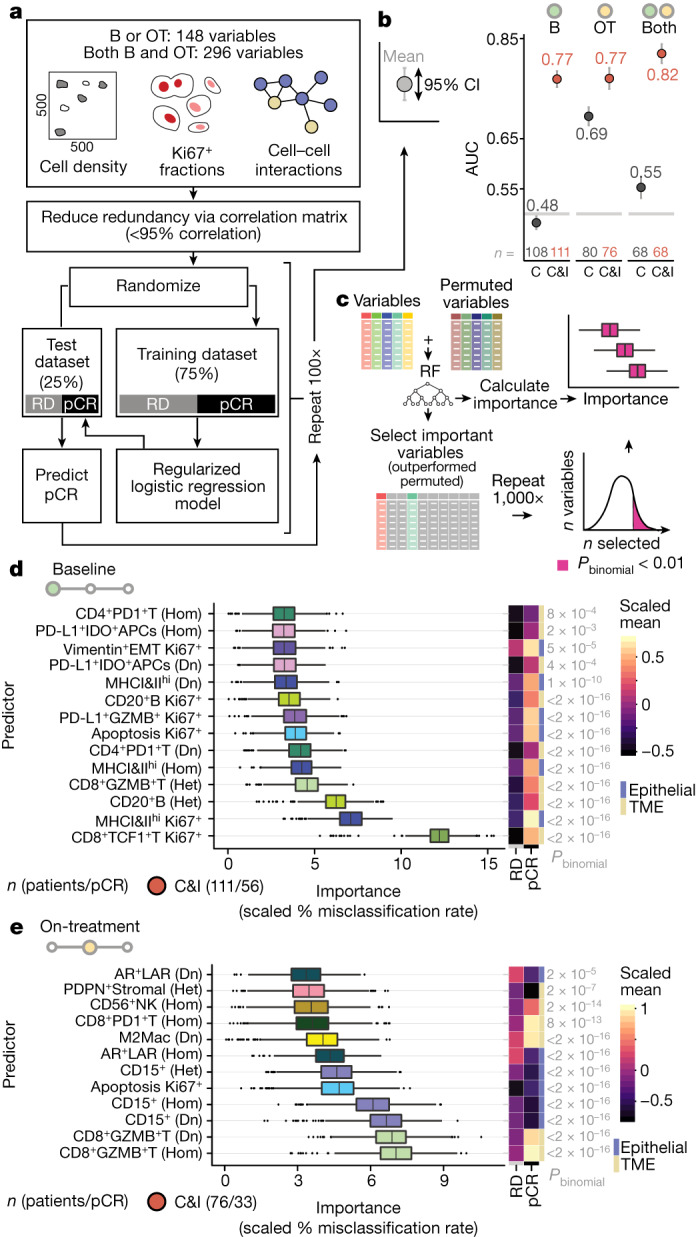
Immune checkpoint blockade (ICB) benefits some patients with triple-negative breast cancer, but what distinguishes responders from non-responders is unclear1. Because ICB targets cell-cell interactions2, we investigated the impact of multicellular spatial organization on response, and explored how ICB remodels the tumour microenvironment. We show that cell phenotype, activation state and spatial location are intimately linked, influence ICB effect and differ in sensitive versus resistant tumours early on-treatment. We used imaging mass cytometry3 to profile the in situ expression of 43 proteins in tumours from patients in a randomized trial of neoadjuvant ICB, sampled at three timepoints (baseline, n = 243; early on-treatment, n = 207; post-treatment, n = 210). Multivariate modelling showed that the fractions of proliferating CD8+TCF1+T cells and MHCII+ cancer cells were dominant predictors of response, followed by cancer-immune interactions with B cells and granzyme B+ T cells. On-treatment, responsive tumours contained abundant granzyme B+ T cells, whereas resistant tumours were characterized by CD15+ cancer cells. Response was best predicted by combining tissue features before and on-treatment, pointing to a role for early biopsies in guiding adaptive therapy. Our findings show that multicellular spatial organization is a major determinant of ICB effect and suggest that its systematic enumeration in situ could help realize precision immuno-oncology.
© 2023. The Author(s).
Conflict of interest statement
C.-S.H. has received research grants for his institution from Aston Sci, AstraZeneca, Daiichi Sankyo, EirGenix, Eli Lilly, Gilead, MSD, Novartis, OBI Pharma, Pfizer, Roche and Seagen; honoraria for speakers’ bureaus from AstraZeneca, Daiichi Sankyo, Eli Lilly, Novartis, Pfizer and Roche; support for attending meetings from Pfizer; and has served on Advisory Boards for AstraZeneca, Daiichi Sankyo, Eli Lilly, Novartis, Pfizer and Roche. D.E. has received consulting fees from AstraZeneca, Daichii Sankyo, Gilead, Novartis, MSD, Roche, Pfizer and Seagen; honoraria for lectures from Amgen, AstraZeneca, Daichii Sankyo, Novartis, MSD, Roche and Pfizer; and support for attending meetings from Pfizer and Roche. B.B. has received honoraria for speaker bureaus from MDS, Roche, Novartis, Pfizer, Palex, AstraZeneca and Lilly; and has served on advisory boards for MSD, Roche and Daichii Sankyo. C.Z. has received grants from Eisai, Pharmamar, Eli Lilly, Celgene, MSD, GSK, Amgen and Daichii Sankyo, and for him and his institution from Roche, Novartis, AstraZeneca, Pfizer, Tesaro, Pierre Fabre, Ist. Gentili, Teva and Seagen; support for attending meetings from Roche, Novartis, Pfizer, Pharmamar, Tesaro, Pierre Fabre, Ist. Gentili and Celgene; has served on advisory boards for Roche, Eisai, Novartis, AstraZeneca, Pfizer, Pharmamar, Amgen, Tesaro, QuintilesIMS, Eli Lilly, Celgene, MSD, GSK and Daichii Sankyo; and has received other financial and non-financial interests from Roche, Novartis, AstraZeneca, Pfizer, Amgen, Tesaro, QuintilesIMS, MSD, GSK and Daichii Sankyo. M.T. has received research grants from Endomag and Exact Sciences; trial honoraria from AstraZeneca, Biom’Up, Celgene, Clearcut, Novartis, pfm medical, Roche and RTI Surgical; honoraria for speakers’ bureaus from Amgen, Art Tempi, AstraZeneca, Clovis, Connect Medica, Eisai, Exact Sciences, Gedeon Richter, Gilead Science, GSK, Hexal, I-Med-Institute, Jörg Eickeler, Laborarztpraxis Walther et al., Lilly, MCI, Medscape, MSD, Medtronic, Novartis, Onkowissen, Pfizer, pfm medical, Roche, Seagen, Streamed Up, Sysmex, Vifor and Viatris; support for attending meetings from Amgen, Art Tempi, AstraZeneca, Clearcut, Clovis, Connect Medica, Daiichi Sankyo, Eisai, Exact Sciences, Hexal, I-Med-Institute, Lilly, MCI, Medtronic, MSD, Norgine, Novartis, Pfizer, pfm Medical, Roche, RTI Surgical and Seagen; has served on advisory boards for Agendia, Amgen, AstraZeneca, Aurikamed, Becton/Dickinson, Biom’Up, ClearCut, Clovis, Daiichi Sankyo, Eisai, Exact Sciences, Gilead Science, Grünenthal, GSK, Lilly, MSD, Norgine, Neodynamics, Novartis, Onkowissen, Organon, Pfizer, pfm Medical, Pierre Fabre, Roche, RTI Surgical, Seagen, Sirius Medical and Sysmex; has received trial funding from Amgen, ClearCut, Clovis, pfm medical, Roche and Servier; and has received Congress support from Amgen, AstraZeneca, Celgene, Daiichi Sankyo, Hexal, Neodynamics, Novartis, Pfizer and Roche. A.A. has received consulting fees from Daichii Sankyo, Roche, Pfizer and Bayer Spain; payment for expert testimony from Pfizer; has served on Advisory Boards for Lilly and Gilead; and has received other services from GSK. E.M.C. has received consulting fees from Roche, Lilly, AstraZeneca, Daiichi Sankyo, Novartis, Pfizer and MSD; honoraria for speakers’ bureaus from Lilly and Roche; and support for attending meetings from Pfizer and Roche. R.G. has received consulting fees from Celgene, Novartis, Roche, BMS, Takeda, Abbvie, AstraZeneca, Jaanssen, MSD, Merk, Gilead, Daiichi Sankyo and Sanofi; support for attending meetings from Roche, Amgen, Janssen, AstraZeneca, Novartis, MSD, Celgene, Gilead, BMS, Abbvie and Daiichi Sankyo; has served on Advisory Boards for Celgene, Novartis, Roche, BMS, Takeda, Abbvie, AstraZeneca, Jaanssen, MSD, Merk, Gilead, Daiichi Sankyo and Sanofi; and has received other financial or non-financial interests from Celgene, Roche, Merk, Takeda, AstraZeneca, Novartis, Amgen, BMS, MSD, Sandoz, Abbvie, Gilead, Daiichi Sankyo, Eli Lilly and Novo Nordisk. B.G. was supported by the National Research, Development, and Innovation Office (PharmaLab, RRF-2.3.1-21-2022-00015). M.C. has received a research grant from Roche. C.M.K. has received grants from the Mater Foundation and HRB Grant/Hospital Co investment and from the Irish Cancer Society; honoraria for educational events from Exact Sciences, AstraZeneca and Daiichi Sankyo; support for attending meetings from Roche; and has participated in Steering Committees for the PALLAS trial, the PenelopeB trial and Destiny Breast 11. L.D.M. has received honoraria for speakers’ bureaus from Roche, Novartis, Eli Lilly, MDS, Pfizer, Ipsen and from Novartis for her institution; support for attending meetings from Roche, Pfizer, Celgene, AstraZeneca and Daiichi Sankyo; and has served on advisory boards for Roche, Eli Lilly, Novartis, MSD, Pfizer, Genomic Health, Pierre Fabre, Daiichi Sankyo, Seagen, Gilead, Exact Sciences, GSK and Agendia. R.S.S. is an employee, stockholder and patent holder of Oncocyte, Inc. G.V. has received grants from Roche/Genentech and AstraZeneca for his institution; consulting fees from Roche/Genentech, AstraZeneca, MDS Oncology and Daiichi Sankyo; honoraria for lectures from Roche/Genentech, AstraZeneca and Daiichi Sankyo; support for attending meetings from Roche/Genentech; and has served on Advisory Boards for Roche/Genentech, AstraZeneca, Pfizer, MDS Oncology and Novartis. L.G. has received consulting fees from Novartis and Odonate Therapeutics; honoraria for lectures from Roche; and support for attending meetings from Pfizer; is co-inventor of ‘European Patent Application Nos. 12195182.6 and 12196177.5 titled PDL-1 expression in anti-HER2 therapy’—Roche—Issued (no compensation provided); has served on advisory boards for AstraZeneca, Celgene, Genentech, Merk Sharp & Dohme, Roche, Pfizer and Sanofi Aventis; and is Chair of the Breast Cancer Research Committee of Fondazione Michelangelo. G.B. has received consulting fees from Roche, AstraZeneca, Novartis, MSD, Sanofi, Daiichi Sankyo and Exact Science; honoraria for speakers’ bureaus from Roche, Pfizer, AstraZeneca, Lilly, Novartis, Neopharm Israel, MSD, Chugai, Daiichi Sankyo, EISAI and Exact Science; support for attending meetings from Roche, Pfizer and AstraZeneca; and has served on advisory boards for Roche, Pfizer, Daiichi Sankyo, Lilly, MSD, Novartis, AstraZeneca, Genomic Health, EISAI, Gilead and Seagen. The other authors declare no competing interests.
Figures















References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
