

Clinical and imaging factors that can predict contagiousness of pulmonary tuberculosis
- PMID: 37674138
- PMCID: PMC10481505
- DOI: 10.1186/s12890-023-02617-y
Clinical and imaging factors that can predict contagiousness of pulmonary tuberculosis
Abstract
Background: Knowledge on predicting pulmonary tuberculosis (PTB) contagiosity in the hospital admission setting is limited. The objective was to assess clinical and radiological criteria to predict PTB contagiosity.
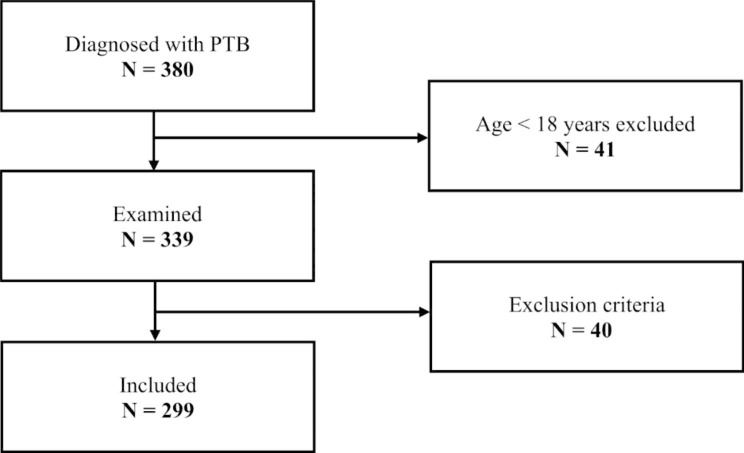
Methods: Retrospective analysis of 7 clinical, 4 chest X-ray (CXR) and 5 computed tomography (CT) signs in 299 PTB patients admitted to an urban tertiary hospital from 2008 to 2016. If the acid fact bacilli stain was positive (AFB+) on admission, the case was considered high contagiosity.
Results: Best predictors for high PTB contagiosity (AFB+) were haemoptysis (OR 4.33), cough (3.00), weight loss (2.96), cavitation in CT (2.75), cavitation in CXR (2.55), tree-in-bud-sign in CT (2.12), German residency of the patient (1.89), and abnormal auscultation findings (1.83). A previous TB infection reduced the risk of contagiosity statistically (0.40). Radiographic infiltrates, miliary picture, and pleural effusion were not helpful in predicting high or low contagiosity. 34% of all patients were clinically asymptomatic (20% of the highly contagious group, 50% of the low contagious group).
Conclusion: Haemoptysis, cough and weight loss as well as cavitation and tree-in-bud sign in CXR/CT can be helpful to predict PTB contagiosity and to improve PTB management.
Keywords: Acid-fast bacilli; Clinical patient management; Disease; Lung infection; Mycobacteria; Prediction.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors have no conflicts of interest to declare.
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
