

Hyperferritinemic sepsis, macrophage activation syndrome, and mortality in a pediatric research network: a causal inference analysis
- PMID: 37674218
- PMCID: PMC10481565
- DOI: 10.1186/s13054-023-04628-x
Hyperferritinemic sepsis, macrophage activation syndrome, and mortality in a pediatric research network: a causal inference analysis
Abstract
Background: One of five global deaths are attributable to sepsis. Hyperferritinemic sepsis (> 500 ng/mL) is associated with increased mortality in single-center studies. Our pediatric research network's objective was to obtain rationale for designing anti-inflammatory clinical trials targeting hyperferritinemic sepsis.
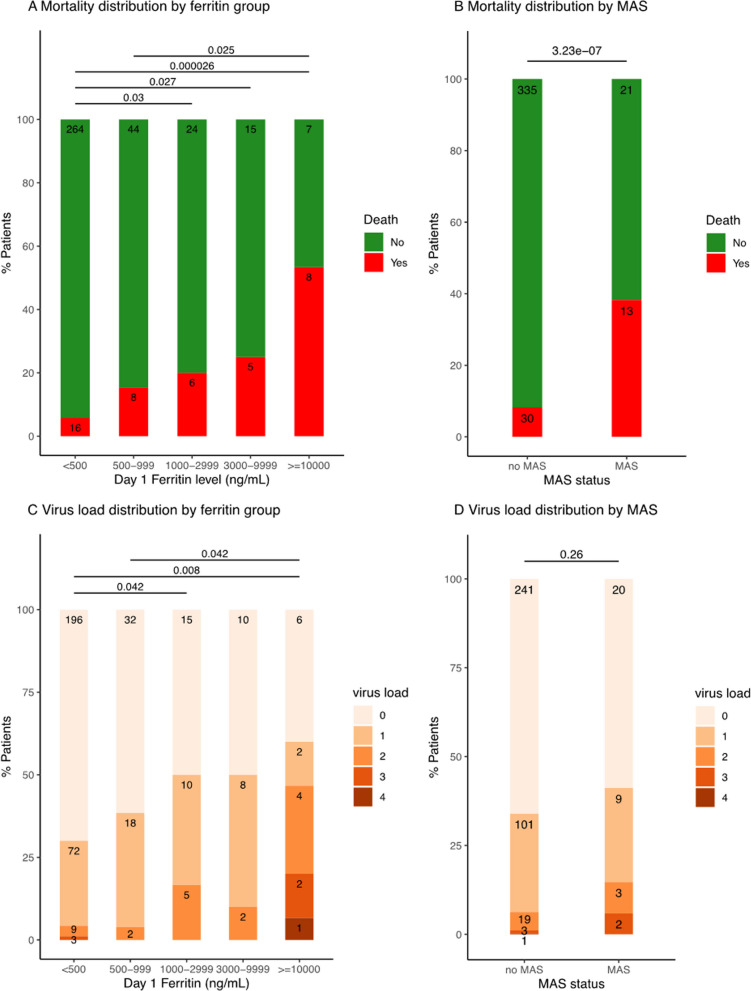
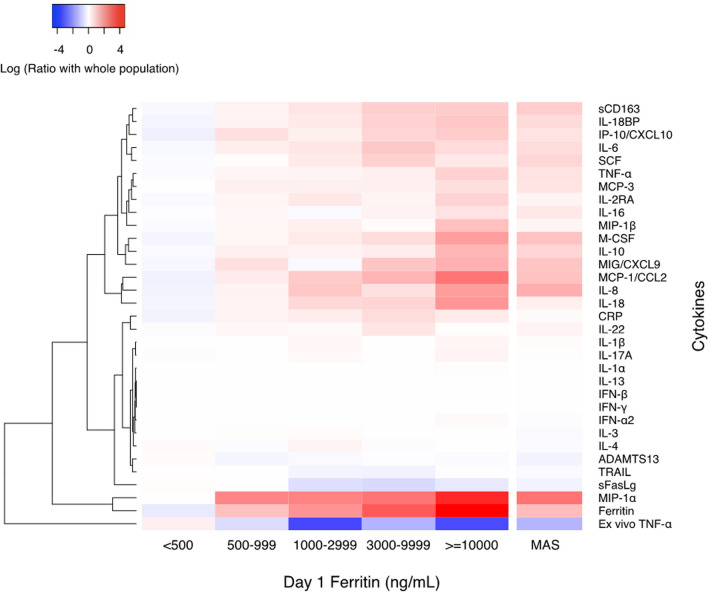
Methods: We assessed differences in 32 cytokines, immune depression (low whole blood ex vivo TNF response to endotoxin) and thrombotic microangiopathy (low ADAMTS13 activity) biomarkers, seven viral DNAemias, and macrophage activation syndrome (MAS) defined by combined hepatobiliary dysfunction and disseminated intravascular coagulation, and mortality in 117 children with hyperferritinemic sepsis (ferritin level > 500 ng/mL) compared to 280 children with sepsis without hyperferritinemia. Causal inference analysis of these 41 variables, MAS, and mortality was performed.
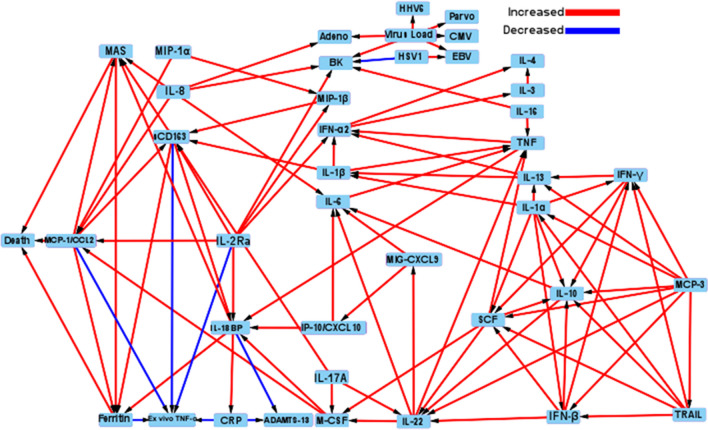
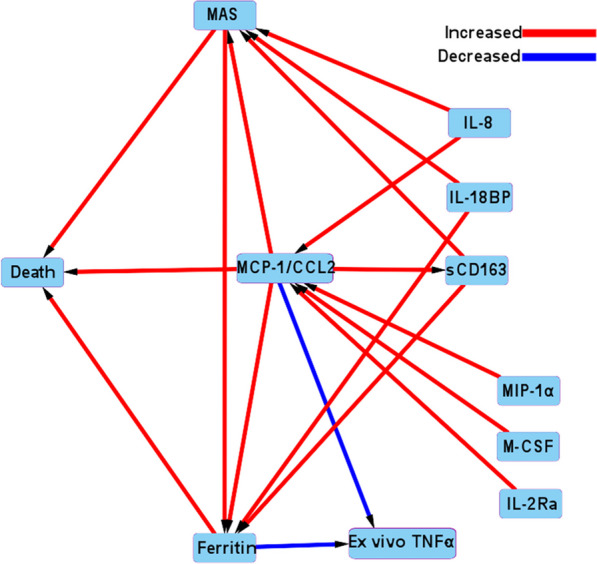
Results: Mortality was increased in children with hyperferritinemic sepsis (27/117, 23% vs 16/280, 5.7%; Odds Ratio = 4.85, 95% CI [2.55-9.60]; z = 4.728; P-value < 0.0001). Hyperferritinemic sepsis had higher C-reactive protein, sCD163, IL-22, IL-18, IL-18 binding protein, MIG/CXCL9, IL-1β, IL-6, IL-8, IL-10, IL-17a, IFN-γ, IP10/CXCL10, MCP-1/CCL2, MIP-1α, MIP-1β, TNF, MCP-3, IL-2RA (sCD25), IL-16, M-CSF, and SCF levels; lower ADAMTS13 activity, sFasL, whole blood ex vivo TNF response to endotoxin, and TRAIL levels; more Adenovirus, BK virus, and multiple virus DNAemias; and more MAS (P-value < 0.05). Among these variables, only MCP-1/CCL2 (the monocyte chemoattractant protein), MAS, and ferritin levels were directly causally associated with mortality. MCP-1/CCL2 and hyperferritinemia showed direct causal association with depressed ex vivo whole blood TNF response to endotoxin. MCP-1/CCL2 was a mediator of MAS. MCP-1/CCL2 and MAS were mediators of hyperferritinemia.
Conclusions: These findings establish hyperferritinemic sepsis as a high-risk condition characterized by increased cytokinemia, viral DNAemia, thrombotic microangiopathy, immune depression, macrophage activation syndrome, and death. The causal analysis provides rationale for designing anti-inflammatory trials that reduce macrophage activation to improve survival and enhance infection clearance in pediatric hyperferritinemic sepsis.
Keywords: Hyperferritinemic sepsis; Immunoparalysis; Macrophage activation syndrome; Multiple organ failure; Severe sepsis; Thrombocytopenia-associated multiple organ failure.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors had no competing interest but they did have the following. Authors Carcillo, Berg, Wessel, Pollack, Meert, Hall, Newth, Doctor, Shanley, Cornell, Harrison, Zuppa, and Dean received support for article research from the NICHD. Dr. Carcillo and Dr Park’s institutions also received funding from the National Institute of General Medical Sciences. Dr. Pollack disclosed that his research is supported by philanthropy from Mallinckrodt Pharmaceuticals. Dr. Hall received funding from LaJolla Pharmaceuticals (service as a consultant), unrelated to the current submission. Dr. Newth received funding from Philips Research North America. Dr. Doctor’s institution received funding from the Department of Defense and Kalocyte. Dr. Shanley received funding from Springer publishing, International Pediatric Research Foundation, and Pediatric Academic Societies. Dr. Cornell disclosed he is co-founder of Pre-Dixon Bio. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Garcia PC, Longhi F, Branco RG, Piva JP, Lacks D, Tasker RC. Ferritin levels in children with severe sepsis and septic shock. Acta Paediatr. 2007;96:1829–1831. - PubMed
-
- Tonial CT, Costa CAD, Andrades GRH, et al. Prediction of poor outcomes for septic children according to ferritin levels in a middle-income setting. Pediatr Crit Care Med. 2020;21:e259–e266. - PubMed
-
- Carcillo JA, Sward K, Halstead ES, et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative pediatric critical care research network investigators: a systemic inflammation mortality risk assessment contingency table for severe sepsis. Pediatr Crit Care Med. 2017;18:143–150. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
