

Opportunistic screening at chest computed tomography: literature review of cardiovascular significance of incidental findings
- PMID: 37675086
- PMCID: PMC10478026
- DOI: 10.21037/cdt-23-79
Opportunistic screening at chest computed tomography: literature review of cardiovascular significance of incidental findings
Abstract
Background and objective: Several incidental cardiovascular findings are present in a routine chest computed tomography (CT) scan, many of which do not make it to the final radiology report. However, these findings have important clinical implications, particularly providing prognosis and risk-stratification for future cardiovascular events. The purpose of this article is to review the literature on these incidental cardiovascular findings in a routine chest CT and inform the radiologist on their clinical relevance.
Methods: A time unlimited review of PubMed and Web of Science was performed by using relevant keywords. Articles in English that involved adults were included.
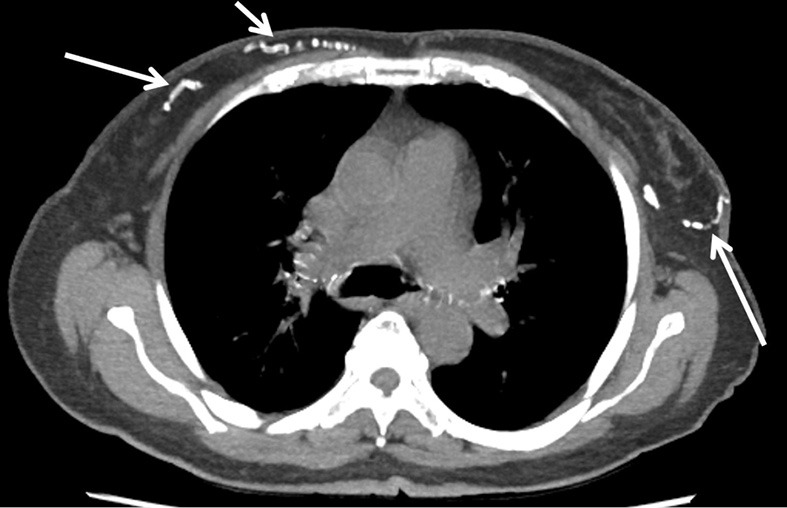
Key content and findings: Coronary artery calcification (CAC) is the most common incidental cardiac finding detected in a routine chest CT and is a significant predictor of cardiovascular events. Noncoronary vascular calcifications in chest CT include aortic valve, mitral annulus, and thoracic aortic calcifications (TAC). Among these, aortic valve calcification (AVC) has the strongest association with coronary artery disease and cardiovascular events. Additional cardiac findings such as myocardial scar and left ventricular size and noncardiac findings such as thoracic fat, bone density, hepatic steatosis, and breast artery calcifications can also help in risk stratification and patient management.
Conclusions: The radiologist interpreting a routine chest CT should be cognizant of the incidental cardiovascular findings, which helps in the diagnosis and risk-stratification of cardiovascular disease. This will guide appropriate referral and management.
Keywords: Chest computed tomography (CT); cardiac; cardiovascular; incidental.
2023 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://cdt.amegroups.com/article/view/10.21037/cdt-23-79/coif). AC and PSR report that they received royalties from Elsevier, unrelated to the content of this manuscript. PSR serves as an unpaid editorial board member of Cardiovascular Diagnosis and Therapy from September 2021 to August 2023. The other authors have no conflicts of interest to declare.
Figures











References
Publication types
LinkOut - more resources
Full Text Sources