

Cardiometabolic predictors of high-risk CCTA phenotype in a diverse patient population
- PMID: 37675408
- PMCID: PMC10477443
- DOI: 10.1016/j.ajpc.2023.100578
Cardiometabolic predictors of high-risk CCTA phenotype in a diverse patient population
Abstract
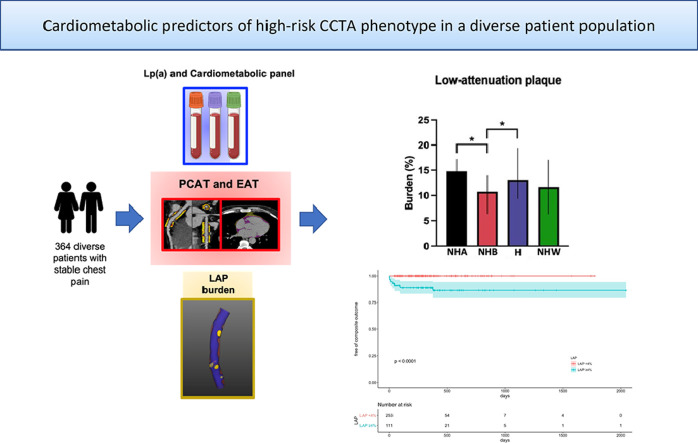
Introduction: Low-attenuation non-calcified plaque (LAP) burden and vascular inflammation by pericoronary adipose tissue (PCAT) measured from coronary CT angiography (CCTA) have shown to be predictors of cardiovascular outcomes. We aimed to investigate the relationships of cardiometabolic risk factors including lipoprotein(a) and epicardial adipose tissue (EAT) with CCTA high-risk imaging biomarkers, LAP and vascular inflammation.
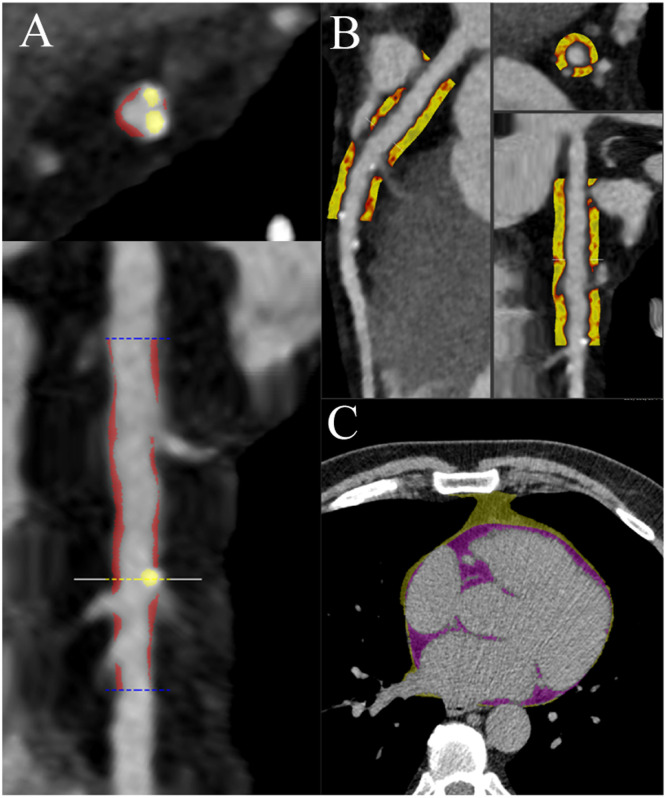
Methods: The patient population consisted of consecutive patients who underwent CCTA for stable chest pain and had a complete cardiometabolic panel including lipoprotein(a). Plaque, PCAT and EAT were measured from CT using semiautomated software. Elevated LAP burden and PCAT attenuation were defined as ≥4% and ≥70.5 HU, respectively. The primary clinical end-point was a composite of myocardial infarction, revascularization or cardiovascular death.
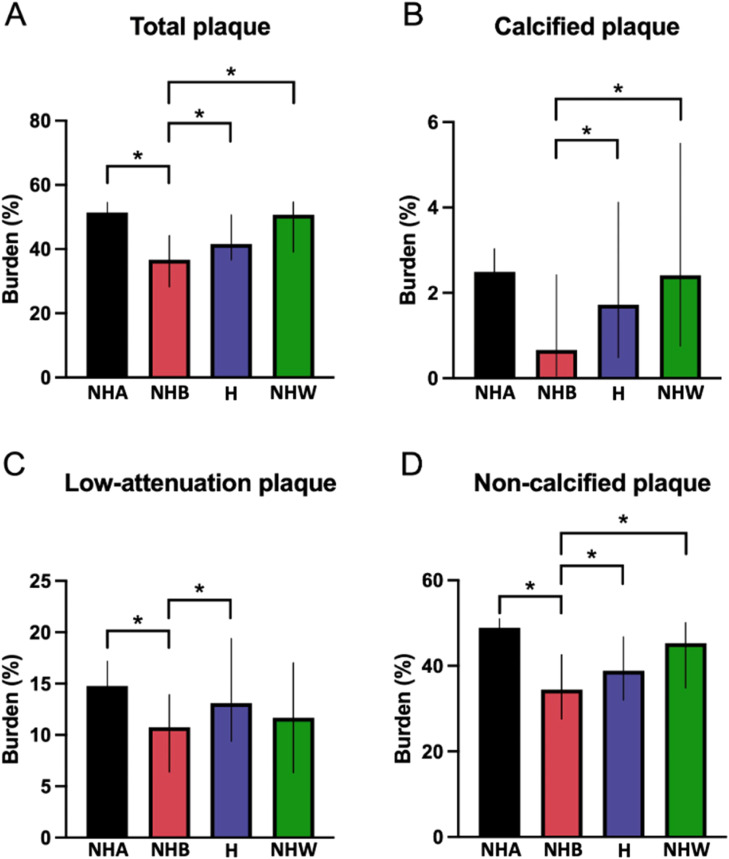
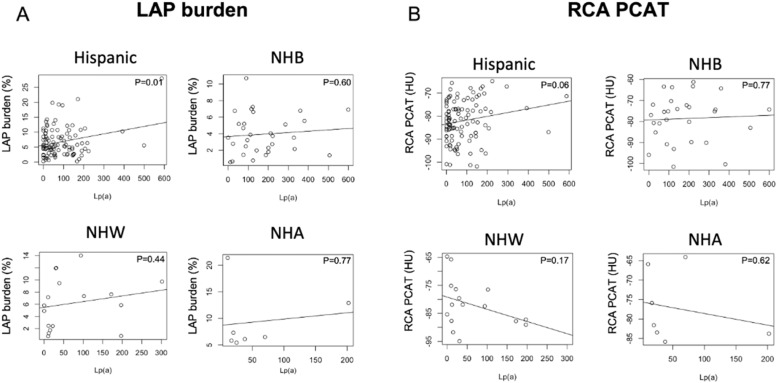
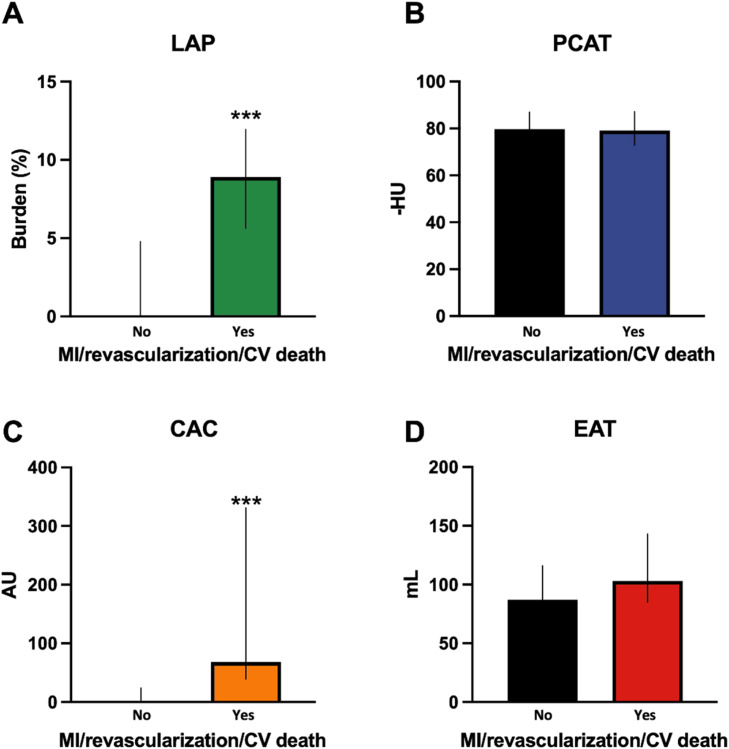
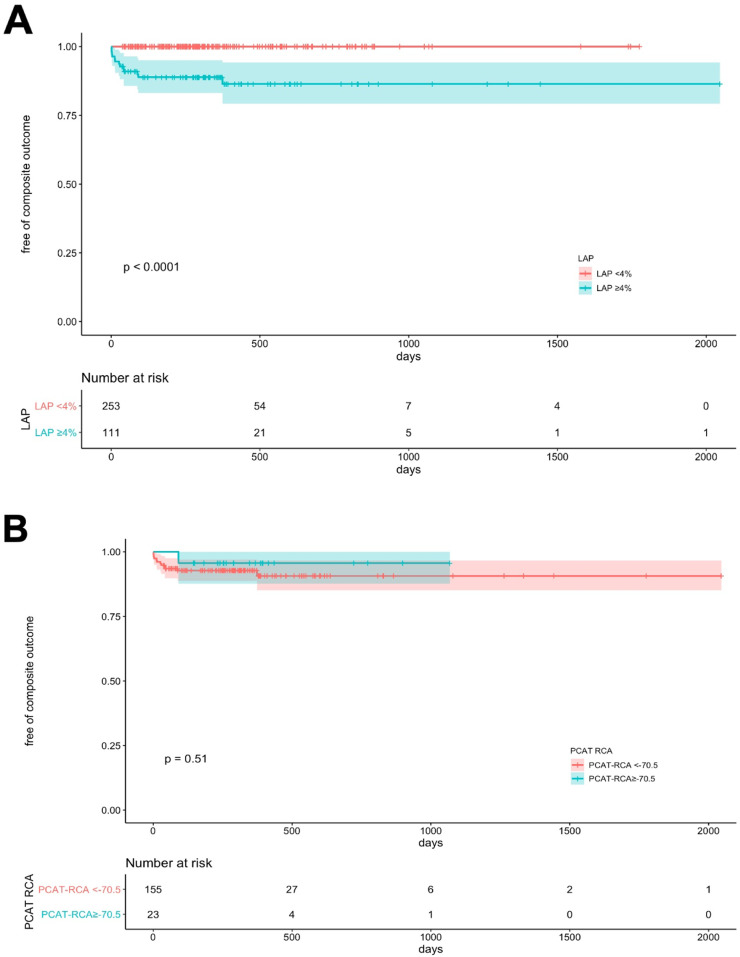
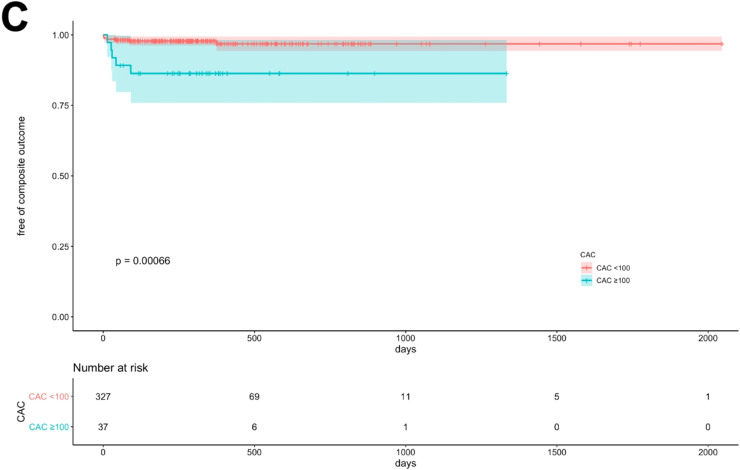
Results: A total of 364 consecutive patients were included (median age 56 years, 64% female); the majority of patients were of Hispanic (60%), and the rest were of non-Hispanic Black (21%), non-Hispanic White (6%) and non-Hispanic Asian (4%) race/ethnicity. The prevalence of elevated LAP burden and PCAT attenuation was 31 and 18%, respectively, while only 8% had obstructive stenosis. There were significant differences in plaque characteristics among different racial/ethnic groups (p<0.001). Lipoprotein(a) correlated with LAP burden in Hispanic patients. Patients with elevated LAP were older, more likely to be have diabetes, hypertension, hyperlipidemia and smoke with higher CAC and EAT volume (all P<0.05). Patients with elevated LAP were more likely to develop the primary clinical outcome (p<0.001) but those with elevated PCAT were not (p=0.797).
Conclusion: The prevalence of LAP and PCAT attenuation were 31 and 18%, respectively. Lipoprotein(a) levels correlated with LAP burden in Hispanic patients. Age, male sex, hypertension and hyperlipidemia increased the odds of elevated LAP, which showed prognostic significance.
Keywords: CT coronary angiogram; Epicardial adipose tissue; High-risk plaque; LAP; PCAT; Risk factors.
© 2023 The Author(s).
Conflict of interest statement
S.V. has received research support from the Department of Veterans Affairs, NIH, Tahir and Jooma Family and Honorarium from American College of Cardiology (Associate Editor for Innovations, acc.org). L.S. has received consulting honorarium from Amgen, BMS and Philips; and Grant support from Amgen. P.J.S, D.S.B. and D.D. have received software royalties from Cedars-Sinai Medical Center. D.D. was supported by grants from National Heart, Lung and Blood institute (1R01HL133616 and 1R01HL148787-01A1). Other authors declare no conflict.
Figures

References
-
- Arnett D.K., Blumenthal R.S., Albert M.A., Buroker A.B., Goldberger Z.D., Hahn E.J., et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American college of cardiology/american heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;74 doi: 10.1016/j.jacc.2019.03.010. - DOI - PMC - PubMed
-
- Tzolos E., Williams M.C., McElhinney P., Lin A., Grodecki K., Flores Tomasino G., et al. Pericoronary adipose tissue attenuation, low-attenuation plaque burden, and 5-year risk of myocardial infarction. JACC Cardiovasc Imaging. 2022;15:1078–1088. doi: 10.1016/j.jcmg.2022.02.004. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
