

Birth spacing and risk of adverse pregnancy and birth outcomes: A systematic review and dose-response meta-analysis
- PMID: 37675816
- PMCID: PMC10619614
- DOI: 10.1111/aogs.14648
Birth spacing and risk of adverse pregnancy and birth outcomes: A systematic review and dose-response meta-analysis
Abstract
Introduction: The association between extreme birth spacing and adverse outcomes is controversial, and available evidence is fragmented into different classifications of birth spacing.
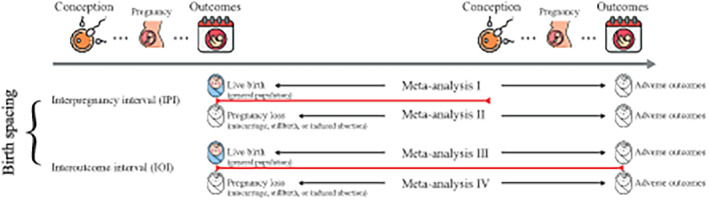
Material and methods: We conducted a systematic review of observational studies to evaluate the association between birth spacing (i.e., interpregnancy interval and interoutcome interval) and adverse outcomes (i.e., pregnancy complications, adverse birth outcomes). Pooled odds ratios (ORs) with 95% confidence intervals (CI) were calculated using a random-effects model, and the dose-response relationships were evaluated using generalized least squares trend estimation.
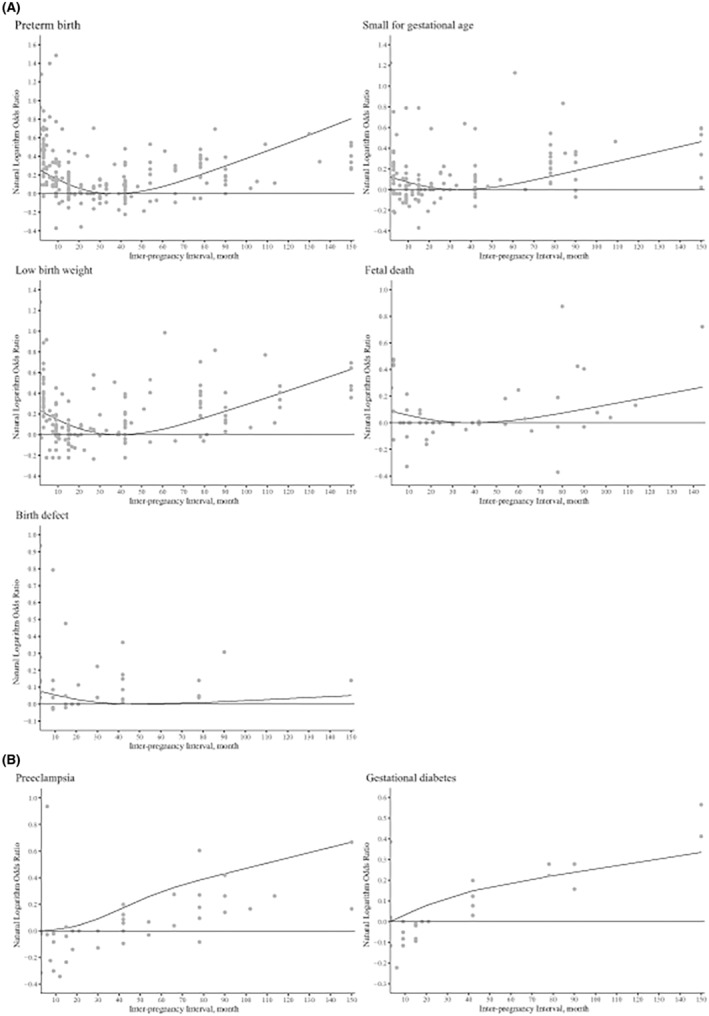
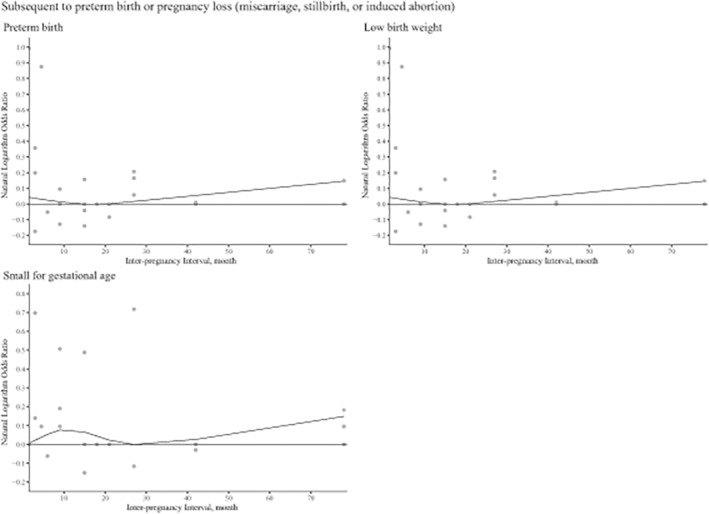
Results: A total of 129 studies involving 46 874 843 pregnancies were included. In the general population, compared with an interpregnancy interval of 18-23 months, extreme intervals (<6 months and ≥ 60 months) were associated with an increased risk of adverse outcomes, including preterm birth, small for gestational age, low birthweight, fetal death, birth defects, early neonatal death, and premature rupture of fetal membranes (pooled OR range: 1.08-1.56; p < 0.05). The dose-response analyses further confirmed these J-shaped relationships (pnon-linear < 0.001-0.009). Long interpregnancy interval was only associated with an increased risk of preeclampsia and gestational diabetes (pnon-linear < 0.005 and pnon-linear < 0.001, respectively). Similar associations were observed between interoutcome interval and risk of low birthweight and preterm birth (pnon-linear < 0.001). Moreover, interoutcome interval of ≥60 months was associated with an increased risk of cesarean delivery (pooled OR 1.72, 95% CI 1.04-2.83). For pregnancies following preterm births, an interpregnancy interval of 9 months was not associated with an increased risk of preterm birth, according to dose-response analyses (pnon-linear = 0.008). Based on limited evidence, we did not observe significant associations between interpregnancy interval or interoutcome interval after pregnancy losses and risk of small for gestational age, fetal death, miscarriage, or preeclampsia (pooled OR range: 0.76-1.21; p > 0.05).
Conclusions: Extreme birth spacing has extensive adverse effects on maternal and infant health. In the general population, interpregnancy interval of 18-23 months may be associated with potential benefits for both mothers and infants. For women with previous preterm birth, the optimal birth spacing may be 9 months.
Keywords: adverse birth outcome; adverse pregnancy outcome; birth interval; interoutcome interval; interpregnancy interval.
© 2023 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
None.
Figures
References
-
- Dorney E, Mazza D, Black KI. Interconception care. Aust J Gen Pract. 2020;49:317‐322. - PubMed
-
- Louis JM, Bryant A, Ramos D, Stuebe A, Blackwell SC. Interpregnancy care. Am J Obstet Gynecol. 2019;220(1):B2‐b18. - PubMed
-
- Organization WH . Report of a WHO Technical Consultation on Birth Spacing: Geneva, Switzerland 13–15 June 2005. World Health Organization; 2007.
-
- Conde‐Agudelo A, Rosas‐Bermúdez A, Kafury‐Goeta AC. Birth spacing and risk of adverse perinatal outcomes: a meta‐analysis. JAMA. 2006;295(15):1809‐1823. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
