

Brain Sagging Dementia
- PMID: 37676440
- PMCID: PMC10590313
- DOI: 10.1007/s11910-023-01297-9
Brain Sagging Dementia
Abstract
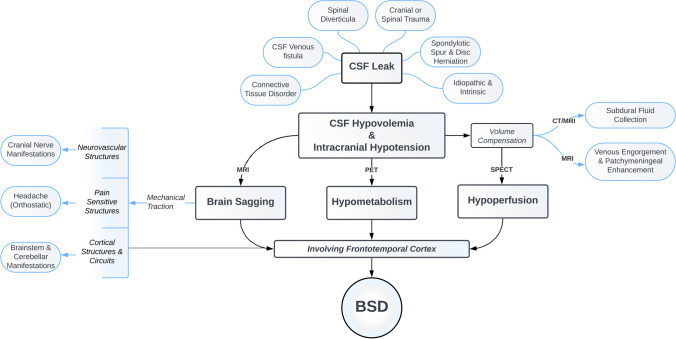
Purpose of review: Brain sagging dementia (BSD) is a rare but devastating form of early-onset dementia characterized by intracranial hypotension and behavioral changes resembling behavioral variant frontotemporal dementia. This review aims to provide a comprehensive overview of BSD, highlighting its pathomechanism, diagnostic tools, and available treatment options.
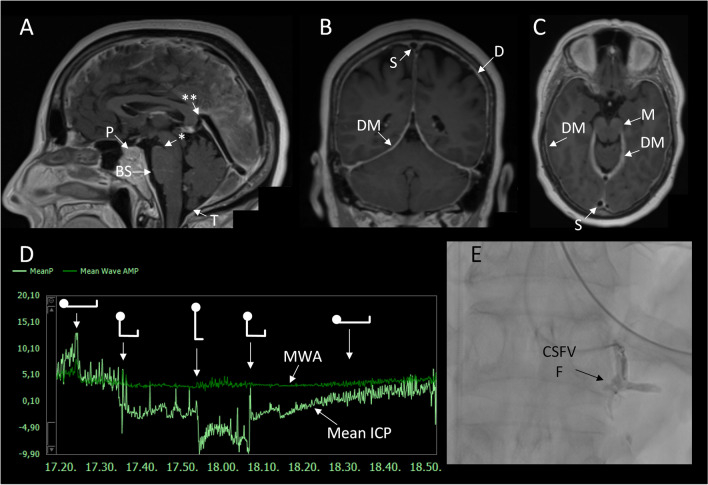
Recent findings: BSD exhibits a complex clinical manifestation with insidious onset and gradual progression of behavioral disinhibition, apathy, inertia, and speech alterations. Additionally, patients may exhibit brainstem and cerebellar signs such as hypersomnolence and gait disturbance. Although headaches are common, they may not always demonstrate typical orthostatic features. Recent radiological advances have improved the detection of CSF leaks, enabling targeted treatment and favorable outcomes. Understanding the pathomechanism and available diagnostic tools for BSD is crucial for a systematic approach to timely diagnosis and treatment of this reversible form of early-onset dementia, as patients often endure a complex and lengthy clinical course.
Keywords: Behavioral variant frontotemporal dementia; Brain sagging dementia (BSD); Early-onset dementia; Intracranial hypotension.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Lashkarivand A, Eide PK. Brain sagging dementia – diagnosis, treatment, and outcome: a review. Neurology. 2022;25:25. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
