

Thiopental and decompressive craniectomy as last-tier ICP-treatments in aneurysmal subarachnoid hemorrhage: is functional recovery within reach?
- PMID: 37676578
- PMCID: PMC10485091
- DOI: 10.1007/s10143-023-02138-6
Thiopental and decompressive craniectomy as last-tier ICP-treatments in aneurysmal subarachnoid hemorrhage: is functional recovery within reach?
Abstract
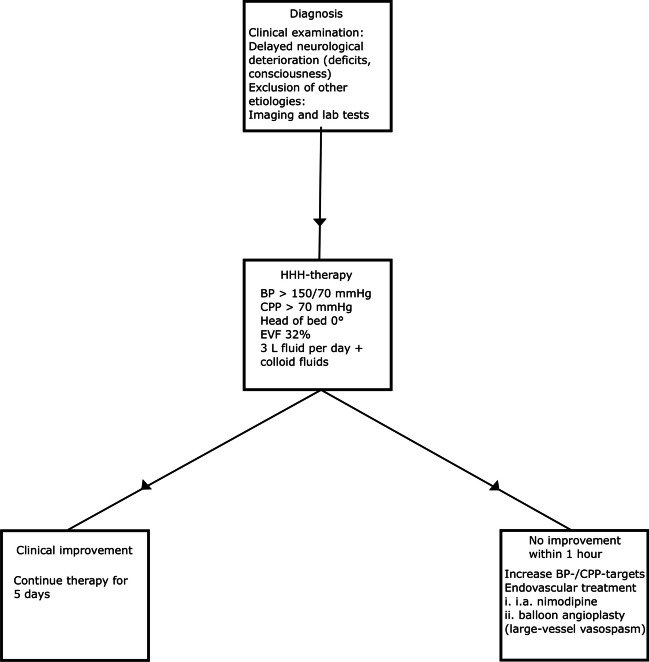
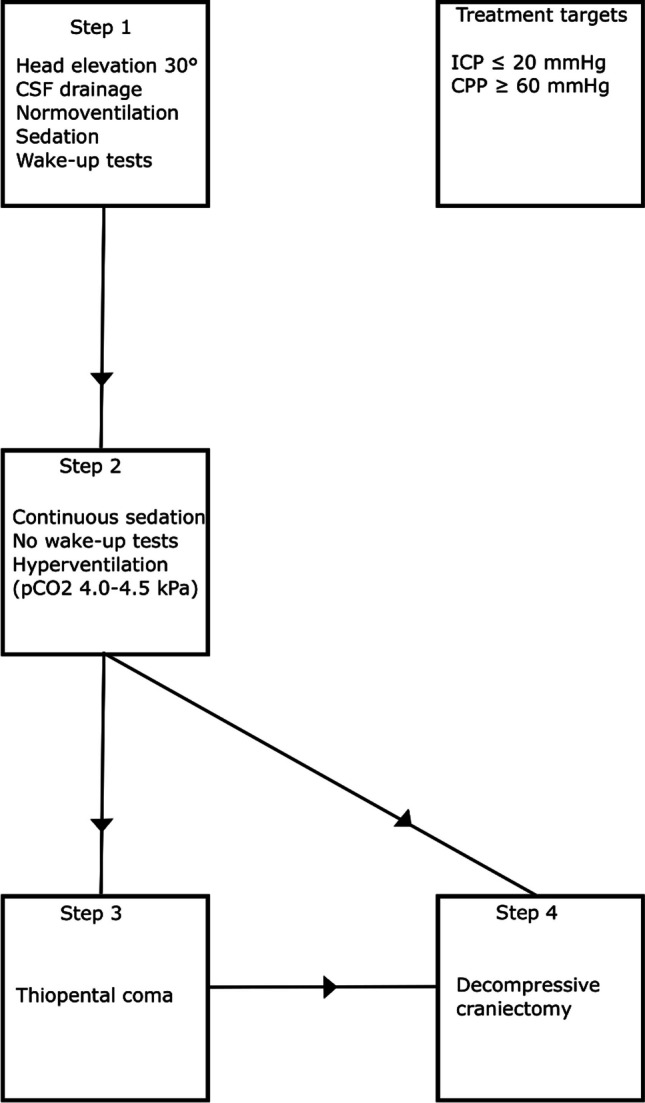
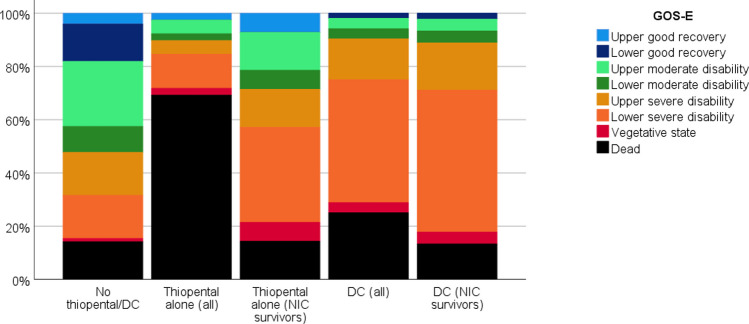
The study aimed to investigate the indication and functional outcome after barbiturates and decompressive craniectomy (DC) as last-tier treatments for elevated intracranial pressure (ICP) in aneurysmal subarachnoid hemorrhage (aSAH). This observational study included 891 aSAH patients treated at a single center between 2008 and 2018. Data on demography, admission status, radiology, ICP, clinical course, and outcome 1-year post-ictus were collected. Patients treated with thiopental (barbiturate) and DC were the main target group.Thirty-nine patients (4%) were treated with thiopental alone and 52 (6%) with DC. These patients were younger and had a worse neurological status than those who did not require these treatments. Before thiopental, the median midline shift was 0 mm, whereas basal cisterns were compressed/obliterated in 66%. The median percentage of monitoring time with ICP > 20 mmHg immediately before treatment was 38%, which did not improve after 6 h of infusion. Before DC, the median midline shift was 10 mm, and the median percentage of monitoring time with ICP > 20 mmHg before DC was 56%, which both significantly improved postoperatively. At follow-up, 52% of the patients not given thiopental or operated with DC reached favorable outcome, whereas this occurred in 10% of the thiopental and DC patients.In summary, 10% of the aSAH cohort required thiopental, DC, or both. Thiopental and DC are important integrated last-tier treatment options, but careful patient selection is needed due to the risk of saving many patients into a state of suffering.
Keywords: Aneurysmal subarachnoid hemorrhage; Decompressive craniectomy; Intracranial pressure; Outcome; Thiopental.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Letter to the editor: thiopental and decompressive craniectomy as last-tier ICP-treatments in aneurysmal subarachnoid hemorrhage: is functional recovery within reach?Neurosurg Rev. 2023 Nov 17;46(1):304. doi: 10.1007/s10143-023-02219-6. Neurosurg Rev. 2023. PMID: 37975924 No abstract available.
References
-
- Alotaibi NM, Elkarim GA, Samuel N, Ayling OGS, Guha D, Fallah A, Aldakkan A, Jaja BNR, de Oliveira Manoel AL, Ibrahim GM, Macdonald RL. Effects of decompressive craniectomy on functional outcomes and death in poor-grade aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J Neurosurg. 2017;127:1315–1325. doi: 10.3171/2016.9.Jns161383. - DOI - PubMed
-
- Brandecker S, Hadjiathanasiou A, Kern T, Schuss P, Vatter H, Güresir E. Primary decompressive craniectomy in poor-grade aneurysmal subarachnoid hemorrhage: long-term outcome in a single-center study and systematic review of literature. Neurosurg Rev. 2021;44:2153–2162. doi: 10.1007/s10143-020-01383-3. - DOI - PMC - PubMed
-
- Carney N, Totten AM, O'Reilly C, Ullman JS, Hawryluk GW, Bell MJ, Bratton SL, Chesnut R, Harris OA, Kissoon N, Rubiano AM, Shutter L, Tasker RC, Vavilala MS, Wilberger J, Wright DW, Ghajar J. Guidelines for the management of severe traumatic brain injury, Fourth Edition. Neurosurgery. 2017;80:6–15. doi: 10.1227/neu.0000000000001432. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
