

doi: 10.1097/TA.0000000000004134.
Epub 2023 Nov 20.
Rethinking limb tourniquet conversion in the prehospital environment
Affiliations
- PMID: 37678162
- PMCID: PMC10662576
- DOI: 10.1097/TA.0000000000004134
Item in Clipboard
Rethinking limb tourniquet conversion in the prehospital environment
J Trauma Acute Care Surg.
.
Abstract
We have highlighted the issue of overuse of tourniquets and described why tourniquet conversion and replacement should be taught and done in the prehospital setting.
Figures

Illustrations of life threatening bleeding, clockwise from top left. (1) Pulsatile or steady bleeding from the limb wound. (2) Blood is pooling on the ground. (3) The overlying clothes are soaked in blood. (4) Bandages or makeshift bandages used to cover the wound are ineffective and steadily becoming soaked with blood. (5) Traumatic extremity amputation. (6) There was prior extremity bleeding and the patient is now in shock (unconscious, confused, pale). Reproduced with permission from the from the American College of Surgeons STOP THE BLEED® program.

Limb with minimal injury but a 5-hour tourniquet use, requiring fasciotomy. Tourniquet conversion was indicated.

Limb with minor injury. The only wound was minor shrapnel injury of the soft tissues of the back surface of the right forearm (under the gauze dressing). The tourniquets were applied around 11:00 am . There was no qualified medic nearby who knew what to do with the tourniquets. Evacuation during the day was impossible due to heavy artillery shelling, and the casualty arrived to the stabilization point at 10:30 pm (11.5 hours tourniquet time). There were no signs of massive bleeding, the patient was stable and awake and alert. A detailed examination revealed no other injuries. The right upper limb was cold, there was no distal pulse, there was no sensitivity, there were no active movements, and passive movements were significantly limited. The casualty underwent an amputation. Tourniquet conversion was indicated.
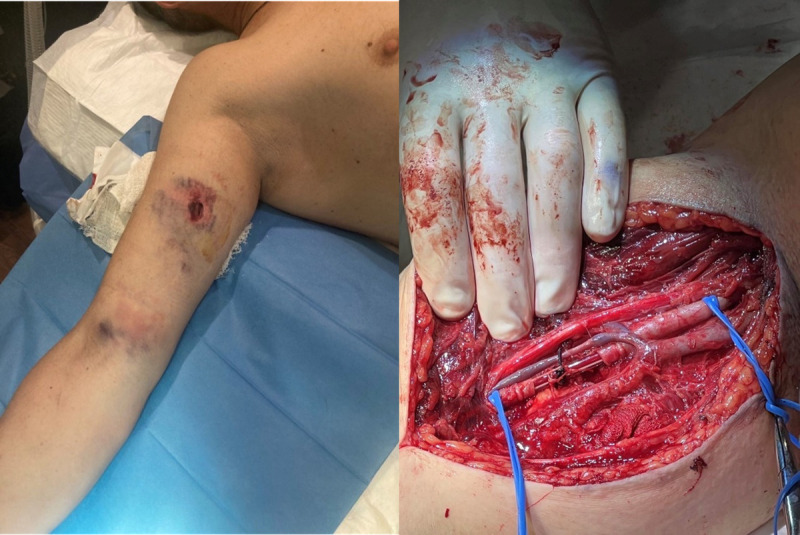
Limb injury with major vascular injury and 5-hour tourniquet use, with brachial artery injury and shunt in place. The tourniquet was just above the wound and likely not amendable to tourniquet conversion or tourniquet replacement.

Limb injury with major vascular injury, tourniquet conversion or tourniquet replacement not attempted as rapid transport to hospital was possible.
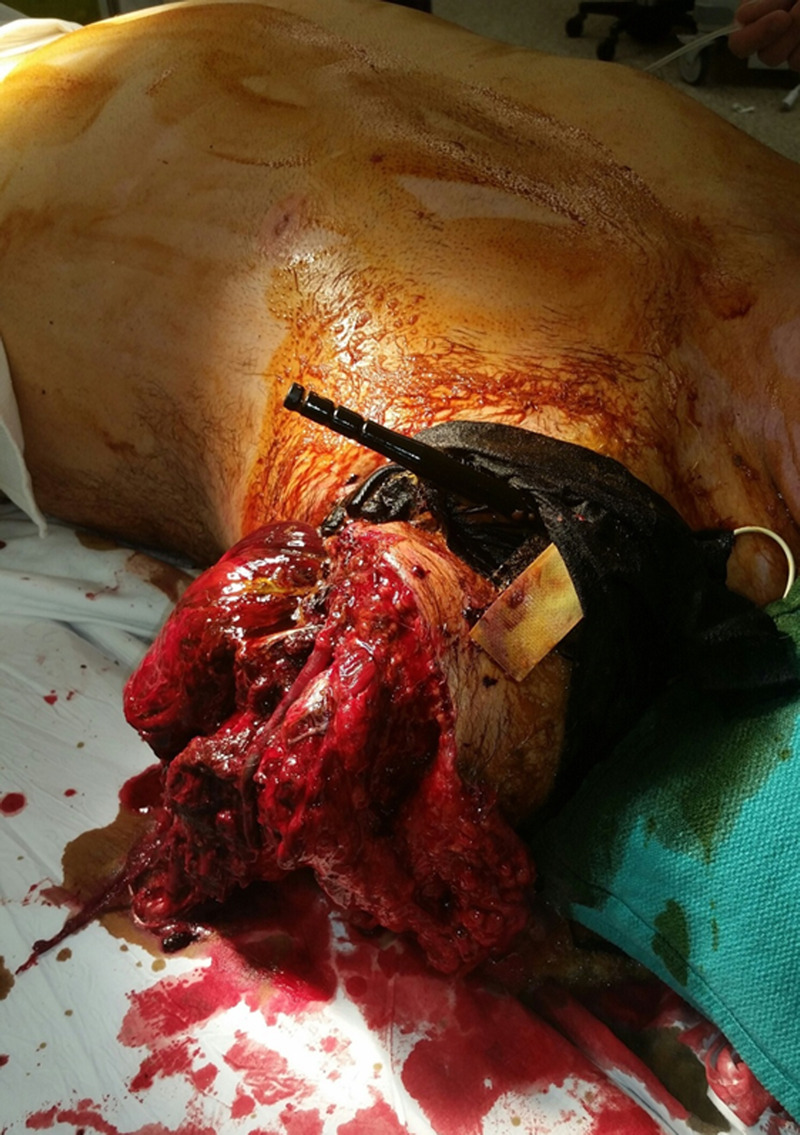
Limb amputation injury with tourniquet in appropriate location. Tourniquet conversion or tourniquet replacement not possible.
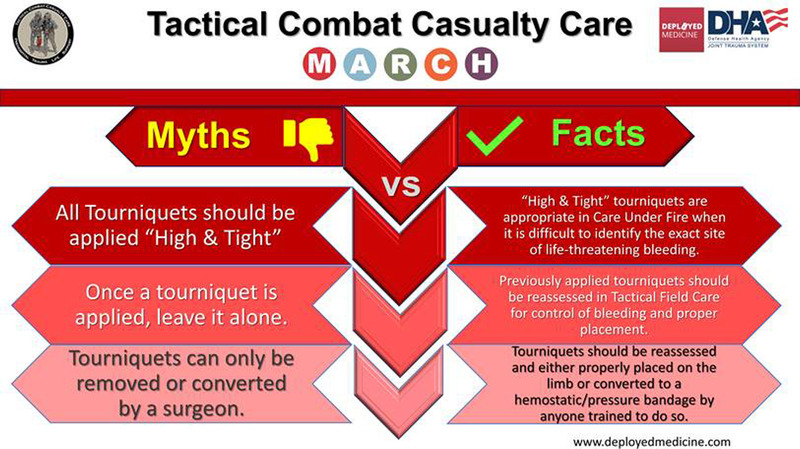
With approval from the Joint Trauma System, Tourniquet Myths and Facts.
References
-
- Wolff LH, Adkins TF. Tourniquet problems in war injuries. Bulletin of the US Army Medical Department. 1945;77–85.
-
- Cosmas Graham A. and Albert E Cowdrey (Eds). (1992). Page 363. The Medical Department - Medical Service in the European Theater of Operations—U.S. Army Center of Military History. Accessed 8 Aug 2023
-
- Mabry RL. Tourniquet use on the battlefield. Mil Med. 2006;171(5):352–356. - PubMed
-
- Mabry RL, Holcomb JB, Baker AM, Cloonan CC, Uhorchak JM, Perkins DE, Canfield AJ, Hagmann JH. United States Army Rangers in Somalia: an analysis of combat casualties on an urban battlefield. J Trauma. 2000;49(3):515–528; discussion 528–529. - PubMed
-
- Butler FK, Jr., Hagmann J, Butler EG. Tactical combat casualty care in special operations. Mil Med. 1996;161(Suppl):3–16. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
