

Moderate to Vigorous Intensity Locomotor Training After Stroke: A Systematic Review and Meta-analysis of Mean Effects and Response Variability
- PMID: 37678805
- PMCID: PMC10843766
- DOI: 10.1097/NPT.0000000000000456
Moderate to Vigorous Intensity Locomotor Training After Stroke: A Systematic Review and Meta-analysis of Mean Effects and Response Variability
Abstract
Background and purpose: This meta-analysis quantified mean effects of moderate to vigorous intensity locomotor training (LT mv ) on walking outcomes in subacute and chronic stroke, and the magnitude of variability in LT mv response.
Methods: Databases were searched for randomized trials comparing LT mv with no intervention, nongait intervention, or low-intensity gait training. Comfortable gait speed (CGS), fastest gait speed (FGS), 6-minute walk test (6MWT), walking activity (steps per day), and adverse effect/event (AE) data were extracted. Pooled estimates were calculated for mean changes, AE relative risks, and the standard deviation of response (SD response ) to LT mv versus control groups, stratified by study chronicity where possible.
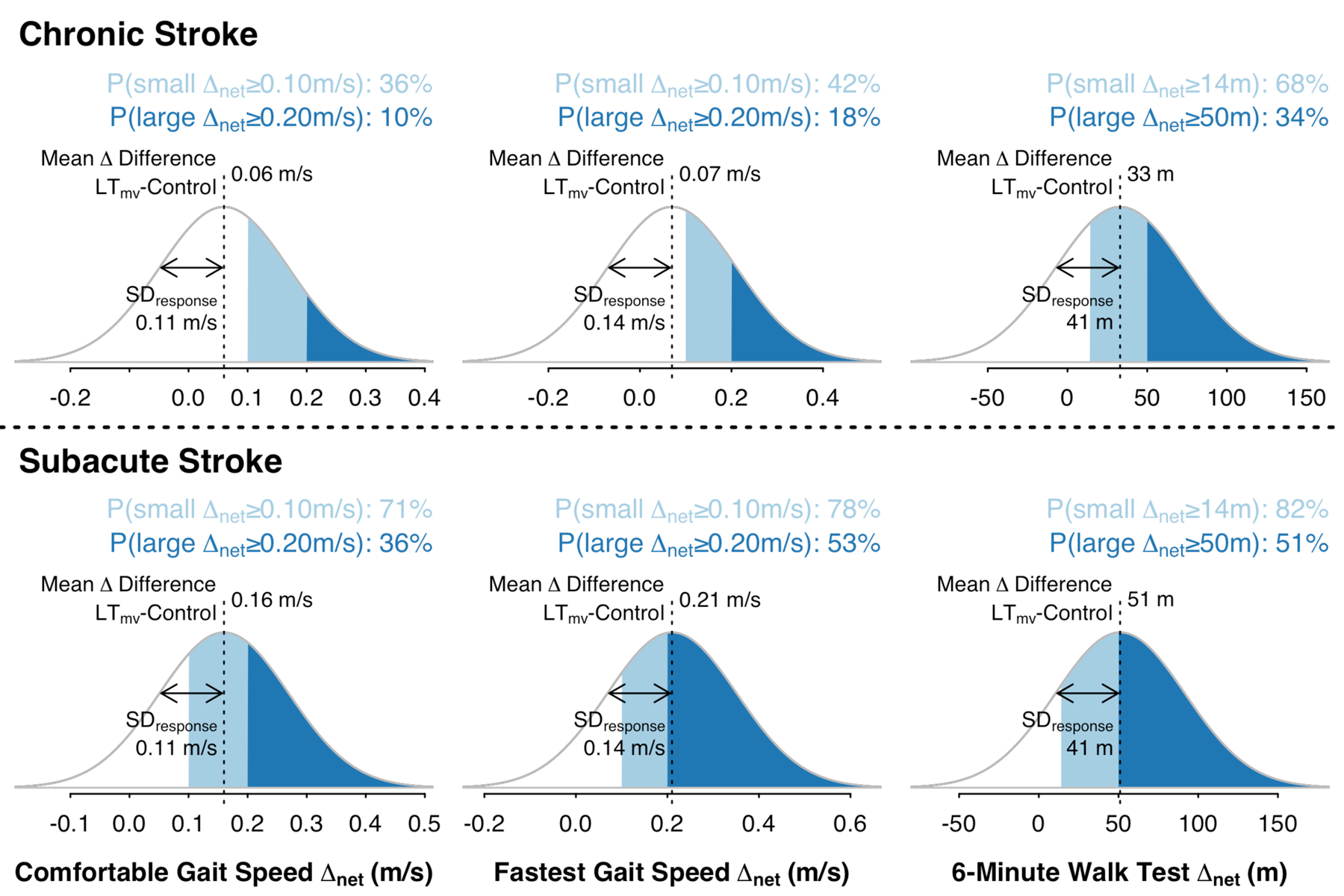
Results: There were 19 eligible studies (total N = 1096): 14 in chronic stroke (N = 839) and 5 in subacute stroke (N = 257). Compared with control interventions, LT mv yielded significantly greater increases in CGS (chronic, +0.06 m/s [95% confidence interval (CI), 0.01-0.10]; subacute, +0.16 [0.12-0.19]; subacute vs chronic, P = 0.03), FGS (chronic, +0.07 m/s [0.02-0.13]; subacute, +0.21 [0.01, 0.41]; P = 0.04), and 6MWT (chronic, +33 m [24-42]; subacute, +51 [26-77]; P = 0.054) but not steps/day (+260 [-1159 to 1679]). There were no treatment-related serious AEs among 398 LT mv participants in 14 AE-reporting studies. SD response estimates indicated substantial response variability: CGS, 0.11 m/s [0.00-0.15]; FGS, 0.14 m/s [-0.00 to 0.20]; and 6MWT, 41 m [27-51].
Discussion and conclusions: LT mv improves mean walking capacity outcomes in subacute and chronic stroke and does not appear to have high risk of serious harm. Response magnitude varies within and between chronicity subgroups, and few studies have tested effects on daily walking activity or non-serious AEs.Video Abstract available for more insights from the authors (see the Video, Supplemental Digital Content 1 available at: http://links.lww.com/JNPT/A452 ).
Copyright © 2023 Academy of Neurologic Physical Therapy, APTA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions version 6.3. Cochrane; 2022:www.training.cochrane.org/handbook.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
