

mRNA COVID-19 Vaccination Does Not Exacerbate Symptoms or Trigger Neural Antibody Responses in Multiple Sclerosis
- PMID: 37679040
- PMCID: PMC10484689
- DOI: 10.1212/NXI.0000000000200163
mRNA COVID-19 Vaccination Does Not Exacerbate Symptoms or Trigger Neural Antibody Responses in Multiple Sclerosis
Abstract
Background and objective: In people with multiple sclerosis (pwMS), concern for potential disease exacerbation or triggering of other autoimmune disorders contributes to vaccine hesitancy. We assessed the humoral and T-cell responses to SARS-CoV-2 after mRNA vaccination, changes in disease activity, and development of antibodies against central or peripheral nervous system antigens.
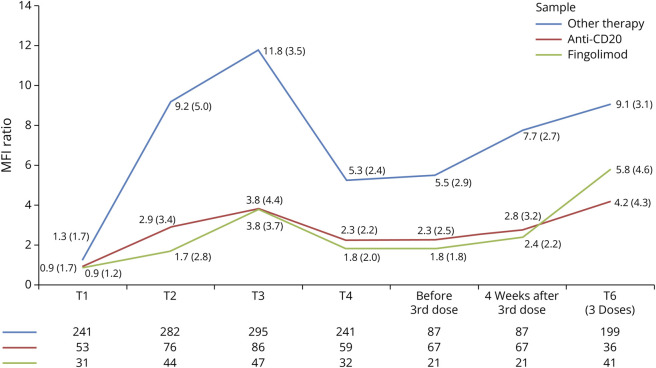
Methods: This was a prospective 1-year longitudinal observational study of pwMS and a control group of patients with other inflammatory neurologic disorders (OIND) who received an mRNA vaccine. Blood samples were obtained before the first dose (T1), 1 month after the first dose (T2), 1 month after the second dose (T3), and 6 (T4), 9 (T5), and 12 (T6) months after the first dose. Patients were assessed for the immune-specific response, annualized relapse rate (ARR), and antibodies to onconeuronal, neural surface, glial, ganglioside, and nodo-paranodal antigens.
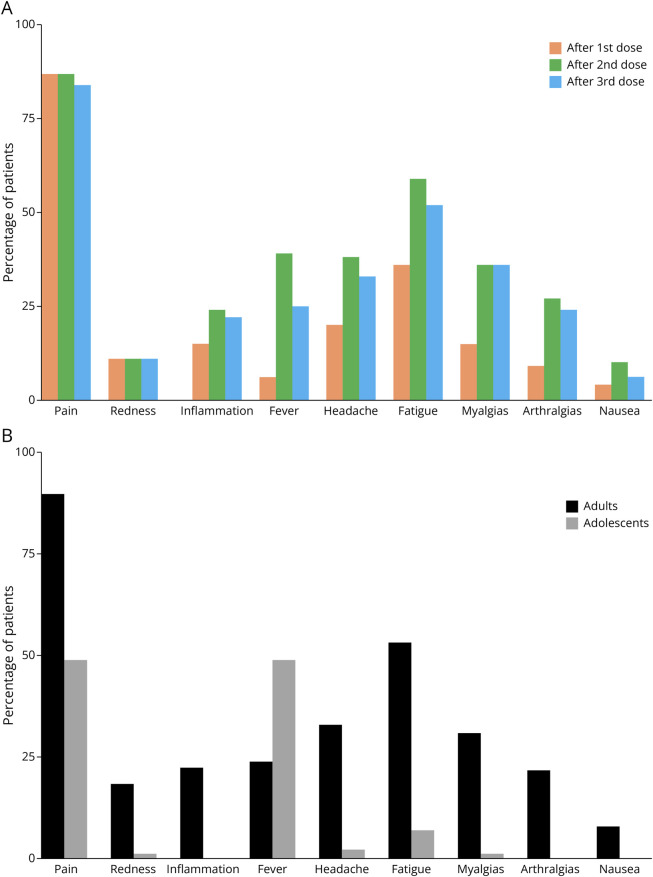
Results: Among 454 patients studied, 390 had MS (22 adolescents) and 64 OIND; the mean (SD) age was 44 (14) years; 315 (69%) were female; and 392 (87%) were on disease-modifying therapies. Antibodies to the receptor-binding domain were detected in 367 (86%) patients at T3 and 276 (83%) at T4. After a third dose, only 13 (22%) of 60 seronegative patients seroconverted, and 255 (92%) remained seropositive at T6. Cellular responses were present in 381 (93%) patients at T3 and in 235 (91%) patients at T6 including all those receiving anti-CD20 therapies and in 79% of patients receiving fingolimod. At T3 (429 patients) or T6 (395 patients), none of the patients had developed CNS autoantibodies. Seven patients had neural antibodies that were already present before immunization (3 adult patients with MS had MOG-IgG, 2 with MG and 1 with MS had neuronal cell surface antibodies [unknown antigen], and 1 with MS had myelin antibody reactivity [unknown antigen]. Similarly, no antibodies against PNS antigens were identified at T3 (427 patients). ARR was lower in MS and not significantly different in patients with OIND. Although 182 (40%) patients developed SARS-CoV-2 infection, no cases of severe COVID-19 or serious adverse events occurred.
Discussion: In this study, mRNA COVID-19 vaccination was safe and did not exacerbate the autoimmune disease nor triggered neural autoantibodies or immune-mediated neurologic disorders. The outcome of patients who developed SARS-CoV-2 infection was favorable.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
Y. Blanco received speaker honoraria from Novartis, Roche, Sanofi, Merck, and Biogen; S. Llufriu received compensation for consulting services and speaker honoraria from Biogen Idec, Novartis, TEVA, Genzyme, Sanofi, Merck, and Bristol-Myers Squibb and holds grants from the Instituto de Salud Carlos III; M. Artola received financial honoraria for presentations and attendance at conferences by Almirall, Biogen idec, Sanofi, Novartis, and Merck; J.M. Cabrera-Maqueda received speaking honoraria and travel expenses for participation in scientific meetings from Sanofi. A. Hernando received financial speaker honoraria from Merck and attendance at conferences by Almirall, Bayer, Biogen, Novartis, Roche, Sanofi, and Teva. J. López-Contreras has received grants from Instituto de Salud Carlos III - Ministry of Economy and Innovation (Spain)and Fundació La Marató, speaking honoraria from Pfizer, MSD, Astra-Zeneca, Guerbet, and Hartmann, funding for clinical trials from Pfizer, Shionogi, MSD, Arsanis, Summit, GSK, Actelion, and Angelini, and for educational activities from MSD, Pfizer, Angelini, Gilead, and Guerbet; L. Martín-Aguilar received speaking honoraria from Roche; E. Martinez-Hernandez received speaking compensation from Biogen; M. Sepulveda received speaking honoraria from Roche, Biogen, and UCB Pharma and travel reimbursement from Biogen, Sanofi, Merck, and Roche for national and international meetings. E. Solana received travel reimbursement and congress assistance from Sanofi and Merck and reports personal fees from Roche Spain; T. Armangué received personal compensation for speaking fees from Sanofi and Roche. J.O. Dalmau holds patents for the use of NMDAR, GABAaR, GABAbR, DPPX, and IgLON5 as autoantibody tests and receives royalties related to autoantibody tests from Athena Diagnostics and Euroimmun Inc. L. Querol received research grants from Instituto de Salud Carlos III - Ministry of Economy and Innovation (Spain), CIBERER, Fundació La Marató, GBS-CIDP Foundation International, UCB, and Grifols, received speaker or expert testimony honoraria from CSL Behring, Novartis, Sanofi-Genzyme, Merck, Annexon, Alnylam, Biogen, Janssen, Lundbeck, ArgenX, UCB, LFB, Octapharma, and Roche, serves at Clinical Trial Steering Committee for Sanofi Genzyme and Roche, and is Principal Investigator for UCB's CIDP01 trial. A. Saiz received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with Merck, Sanofi, Biogen, Roche, Novartis, Janssen, and Horizon Therapeutics. The other authors report no disclosures. Go to
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous