

Autonomy support encourages use of more-affected arm post-stroke
- PMID: 37679781
- PMCID: PMC10483757
- DOI: 10.1186/s12984-023-01238-0
Autonomy support encourages use of more-affected arm post-stroke
Erratum in
-
Correction: Autonomy support encourages use of more-afected arm post-stroke.J Neuroeng Rehabil. 2023 Sep 26;20(1):126. doi: 10.1186/s12984-023-01244-2. J Neuroeng Rehabil. 2023. PMID: 37752533 Free PMC article. No abstract available.
Abstract
Background: Autonomy support, which involves providing individuals the ability to control their own behavior, is associated with improved motor control and learning in various populations in clinical and non-clinical settings. This study aimed to investigate whether autonomy support combined with an information technology (IT) device facilitated success in using the more-affected arm during training in individuals with stroke. Consequently, we examined whether increased success influenced the use of the more-affected arm in mild to moderate subacute to chronic stroke survivors.
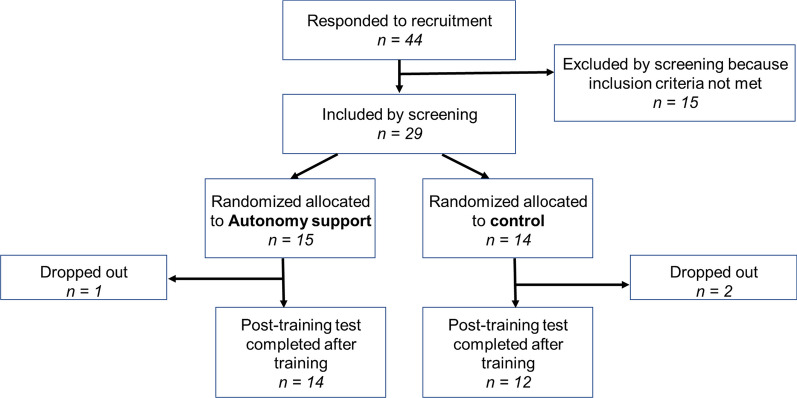
Methods: Twenty-six participants with stroke were assigned to the autonomy support or control groups. Over a 5-week period, training and test sessions were conducted using the Individualized Motivation Enhancement System (IMES), a device developed specifically for this study. In the autonomy support group, participants were able to adjust the task difficulty parameter, which controlled the time limit for reaching targets. The control group did not receive this option. The evaluation of the more-affected arm's use, performance, and impairment was conducted through clinical tests and the IMES. These data were then analyzed using mixed-effect models.
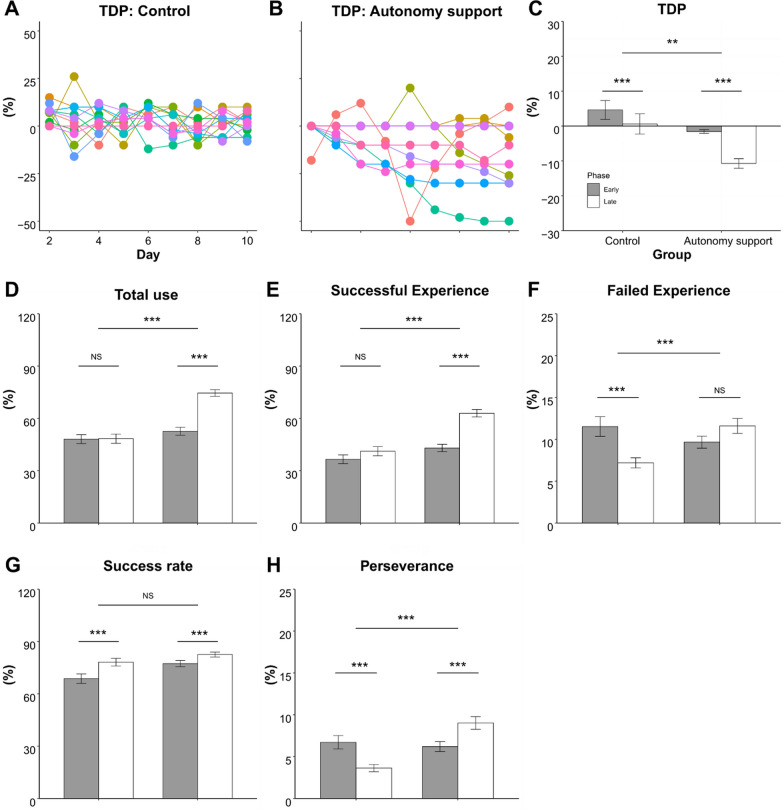
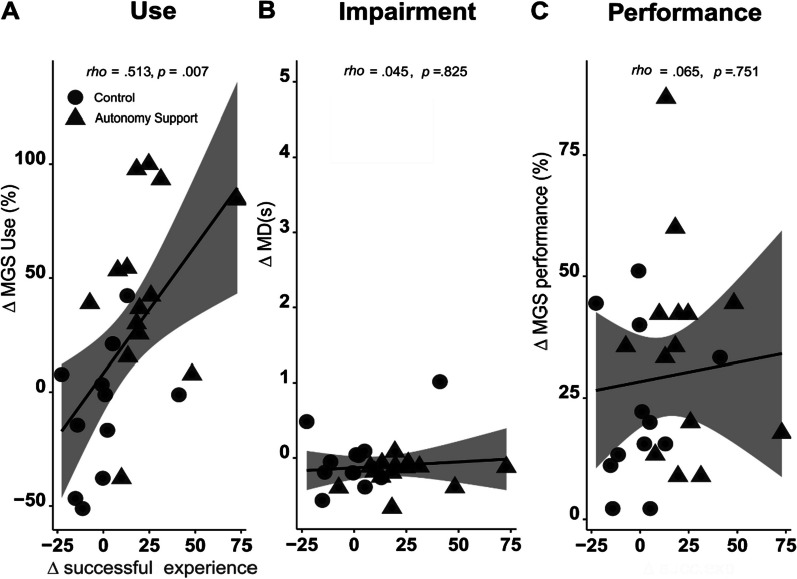
Results: In the IMES test, both groups showed a significant improvement in performance (p < 0.0001) after the training period, without any significant intergroup differences (p > 0.05). However only the autonomy support group demonstrated a significant increase in the use of the more-affected arm following the training (p < 0.001). Additionally, during the training period, the autonomy support group showed a significant increase in successful experiences with using the more-affected arm (p < 0.0001), while the control group did not exhibit the same level of improvement (p > 0.05). Also, in the autonomy support group, the increase in the use of the more-affected arm was associated with the increase in the successful experience significantly (p = 0.007).
Conclusions: Combining autonomy support with an IT device is a practical approach for enhancing performance and promoting the use of the more-affected upper extremity post-stroke. Autonomy support facilitates the successful use of the more-affected arm, thereby increasing awareness of the training goal of maximizing its use.
Trial registration: The study was registered retrospectively with the Clinical Research Information Service (KCT0008117; January 13, 2023; https://cris.nih.go.kr/cris/search/detailSearch.do/23875 ).
Keywords: Choice behavior; Hemiparesis; Motivation; Self-efficacy; Upper extremity.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Taub E, Uswatte G, Mark VW, Morris DM. The learned nonuse phenomenon: Implications for rehabilitation. Eura Medicophys. 2006;42:241–255. - PubMed
-
- Bosch J, O’Donnell MJ, Barreca S, Thabane L, Wishart L. Does task-oriented practice improve upper extremity motor recovery after stroke? A systematic review. ISRN Stroke. 2014;2014:1–10. doi: 10.1155/2014/504910. - DOI
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
