

Head-to-head comparison of the WHO STEPwise approach with immediate unattended and delayed unattended automated blood pressure measurements during household-based screening: a diagnostic accuracy study in Lesotho
- PMID: 37680951
- PMCID: PMC10480531
- DOI: 10.1016/j.eclinm.2023.102197
Head-to-head comparison of the WHO STEPwise approach with immediate unattended and delayed unattended automated blood pressure measurements during household-based screening: a diagnostic accuracy study in Lesotho
Abstract
Background: WHO introduced the STEPwise approach to surveillance (STEPS) to monitor trends in non-communicable diseases. For arterial hypertension, the STEPS protocol takes the average of the last two out of three standard blood pressure measurements (SBPM). This study assesses the diagnostic accuracy of SBPM, same-day and next-day unattended automated measurement (uABP), with 24 h ambulatory measurement (24 h-ABPM) as reference.
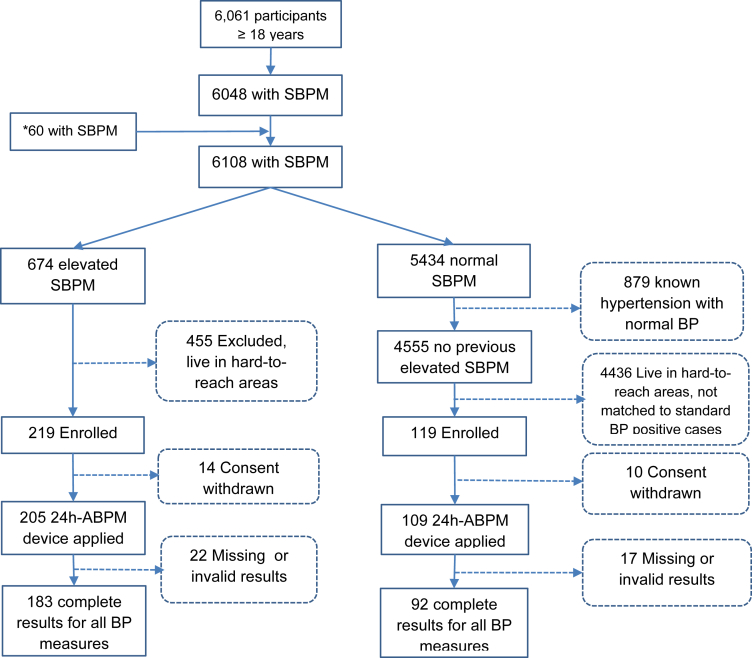
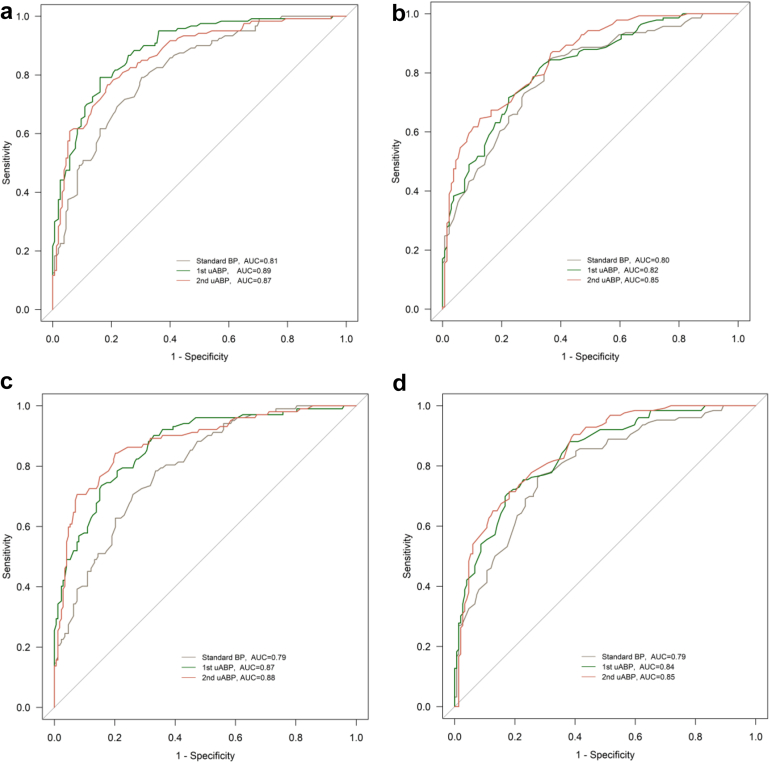
Methods: This diagnostic accuracy study was done within a population-based household survey on cardiovascular risk factors in two districts in Northern Lesotho. Adults (aged ≥ 18 years) with elevated SBPM (defined as ≥140/90 mmHg), and 2:1 age- and sex-matched participants with normal SBPM during the survey were recruited. Following SBPM, first uABP readings were obtained on survey day. Afterwards, participants received a 24 h-ABPM device. Second uABP readings were taken 24 h later, after retrieval of the 24 h-ABPM. The main outcome was overall diagnostic accuracy of all screening measurements (SBPM, first uABP, and second uABP), determined using area under the receiver operating characteristic curve (AUROC), with 24 h-ABPM as a reference.
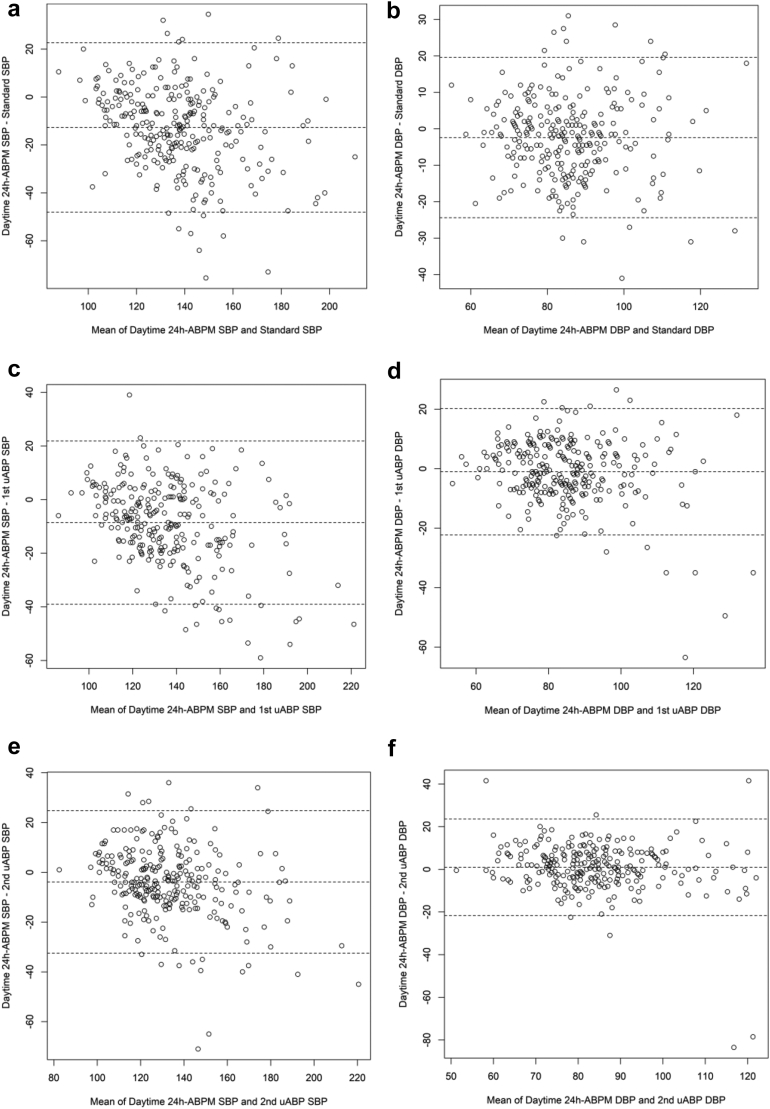
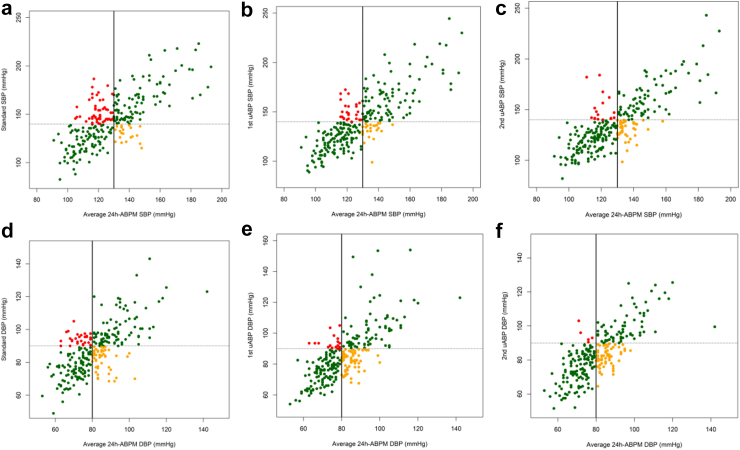
Findings: Between November 2, 2021 and August 31, 2022, 275 participants (mean age 58 years (SD: 16 years), 163 (59%) female) were enrolled, 183 of whom had elevated and 92 had normal SBPM. Mean difference between systolic daytime 24 h-ABPM and screening measurements was highest for SBPM (mean difference: -13 mmHg; 95% CI: -14 to -11). Mean difference between diastolic daytime 24 h-ABPM and diastolic SBPM was -2 mmHg (95% CI: -4 to -1), whereas no difference was found for mean diastolic first uABP (mean difference: -1 mmHg; 95% CI: -2.0 to 0.3); and mean diastolic second uABP (mean difference: 1.0 mmHg; 95% CI: -0.4 to 2.3). White coat hypertension was highest with SBPM (55 [20%]), followed by first uABP (27 [9.8%]), and second uABP (18 [6.5%]). Using systolic daytime 24 h-ABPM as a reference, the uABPs had higher AUROC (first uABP: 87% [95% CI: 83-91]; second uABP: 88% [95% CI: 84-92]); SBPM: (79% [95% CI: 74-85]). This difference was significant between first uABP and SBPM (P = 0.0024), and between second uABP and SBPM (P = 0.0017).
Interpretation: uABP had better diagnostic performance than SBPM. Integration of uABP into STEPS protocol should be considered.
Funding: Swiss Agency for Development and Cooperation under the ComBaCaL project, and the World Diabetes Foundation.
Keywords: Ambulatory blood pressure monitor; Lesotho; STEPS; Sub-Saharan Africa; Survey screen blood pressure; Unattended automated office blood pressure.
© 2023 The Author(s).
Conflict of interest statement
NDL reports grants from the 10.13039/100000001Swiss National Science Foundation (Eccellenza Professorship and project grant), 10.13039/501100011318Botnar Foundation, Botnar Center for Child Health, 10.13039/100009131Swiss Agency for Development and Cooperation, and Moritz Straus Stiftung; consulting fees from 10.13039/100010877ViiV Healthcare, the 10.13039/501100005416Research Council of Norway, and the 10.13039/100000001Swiss National Science Foundation (all paid to his division); honoraria for lectures from ETHZ and Swiss TPH (paid to his division); travel grants from 10.13039/100005564Gilead Sciences and 10.13039/100010877ViiV Healthcare; participation on a Data Safety Monitoring Board for Pharming (payments made to his division). EF received travel support from the European Union’s Horizon 2020 research and innovation programme under Marie Skłodowska-Curie grant agreement (No 801076), through SSPH+ Global PhD Fellowship Programme in Public Health Sciences (GlobalP3HS). All other authors declare no competing interests.
Figures
References
-
- World Health Organisation Blood pressure/hypertension. 2023. https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3155
-
- Beaney T., Schutte A.E., Stergiou G.S., et al. May measurement month 2019: the global blood pressure screening campaign of the international society of hypertension. Hypertension. 2020;76(2):333–341. - PubMed
-
- Woodiwiss A.J., Gafane-Matemane L.F., Norton G.R., et al. May measurement Month 2019: an analysis of blood pressure screening results from South Africa. Eur Heart J Suppl. 2021;23(Supplement_B):B134–B137.
LinkOut - more resources
Full Text Sources
