

Clonal Hematopoiesis in Clinical and Experimental Heart Failure With Preserved Ejection Fraction
- PMID: 37681311
- PMCID: PMC10575571
- DOI: 10.1161/CIRCULATIONAHA.123.064170
Clonal Hematopoiesis in Clinical and Experimental Heart Failure With Preserved Ejection Fraction
Abstract
Background: Clonal hematopoiesis (CH), which results from an array of nonmalignant driver gene mutations, can lead to altered immune cell function and chronic disease, and has been associated with worse outcomes in patients with heart failure (HF) with reduced ejection fraction. However, the role of CH in the prognosis of HF with preserved ejection fraction (HFpEF) has been understudied. This study aimed to characterize CH in patients with HFpEF and elucidate its causal role in a murine model.
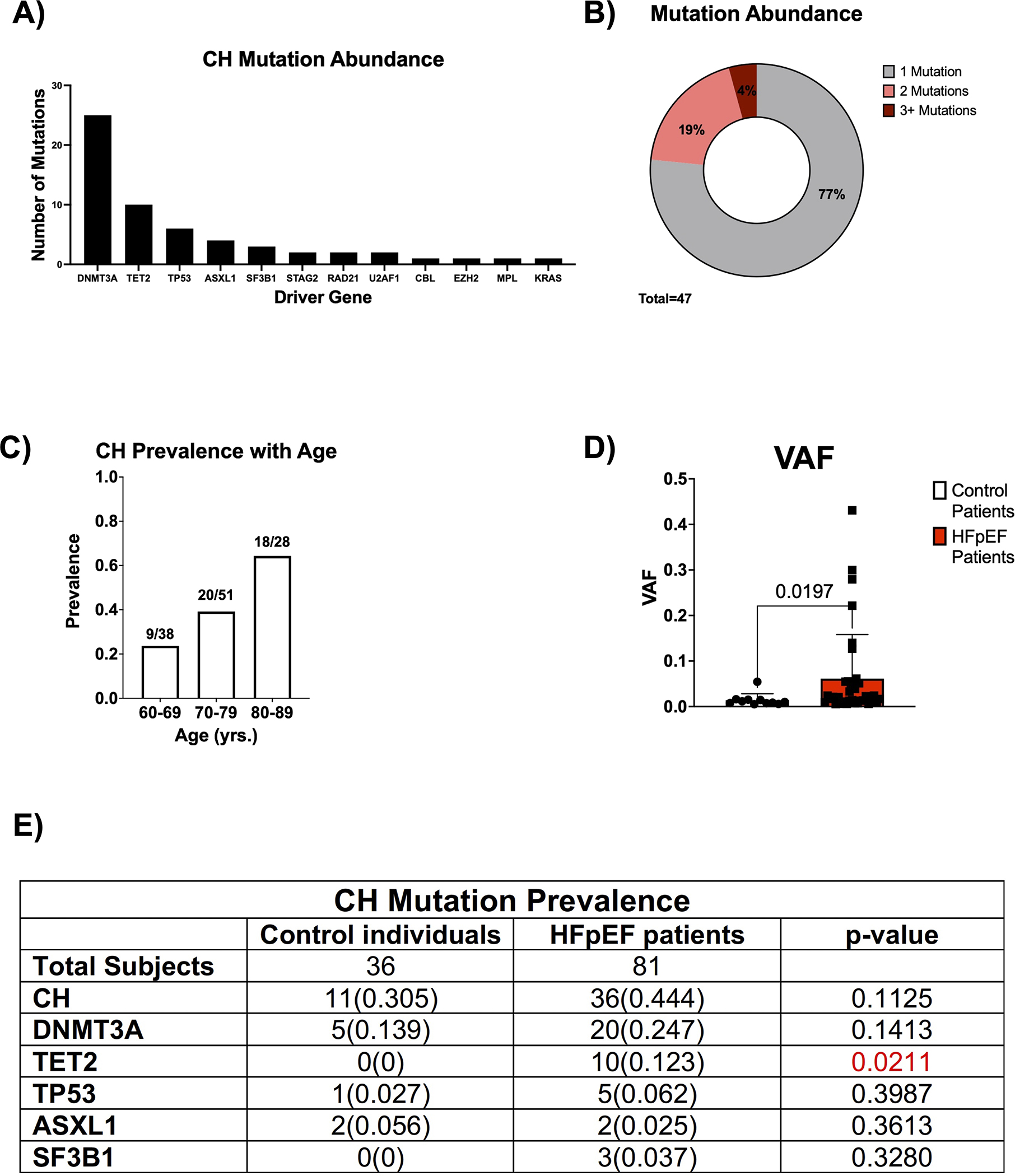
Methods: Using a panel of 20 candidate CH driver genes and a variant allele fraction cutoff of 0.5%, ultradeep error-corrected sequencing identified CH in a cohort of 81 patients with HFpEF (mean age, 71±6 years; ejection fraction, 63±5%) and 36 controls without a diagnosis of HFpEF (mean age, 74±7 years; ejection fraction, 61.5±8%). CH was also evaluated in a replication cohort of 59 individuals with HFpEF.
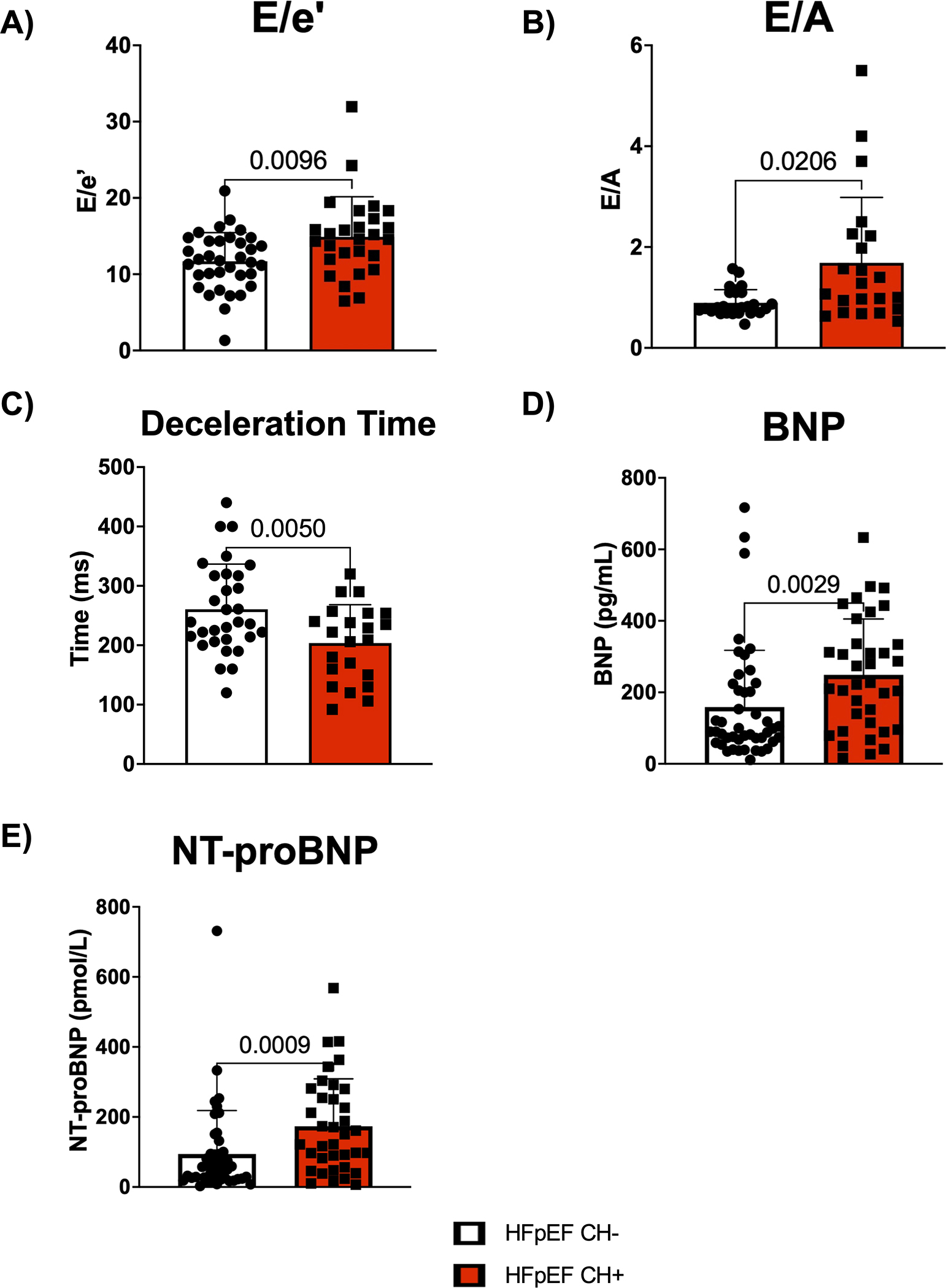
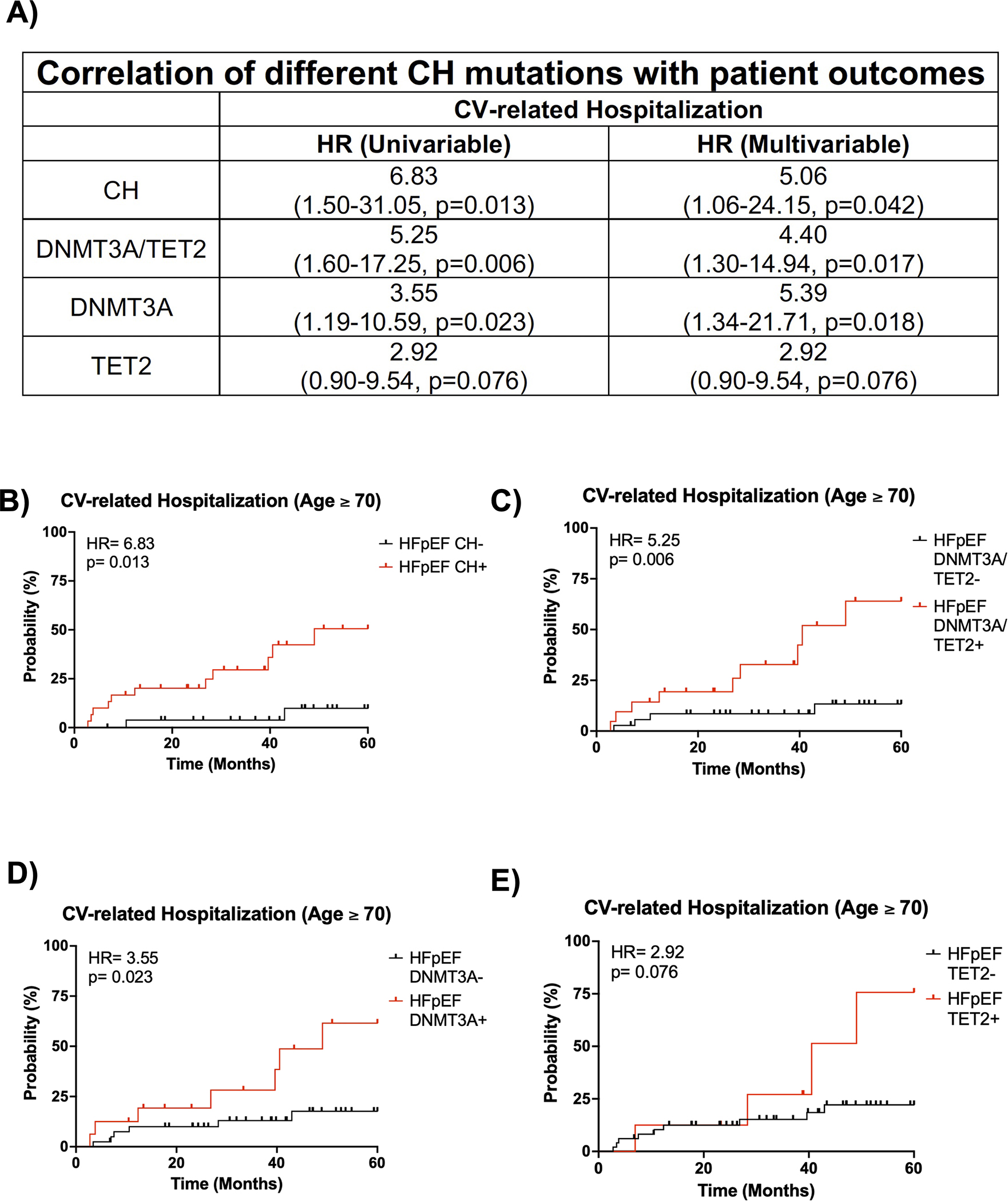
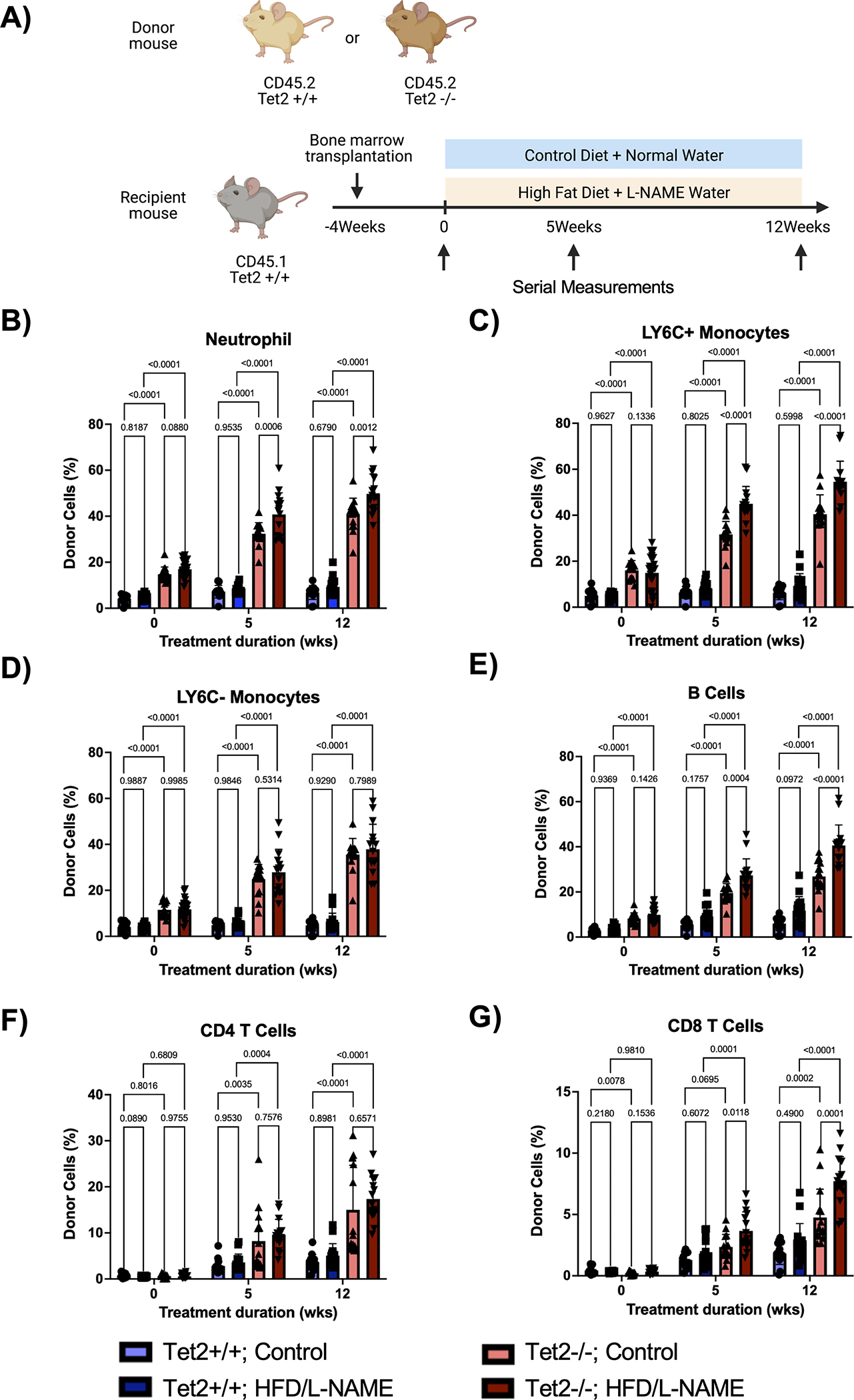
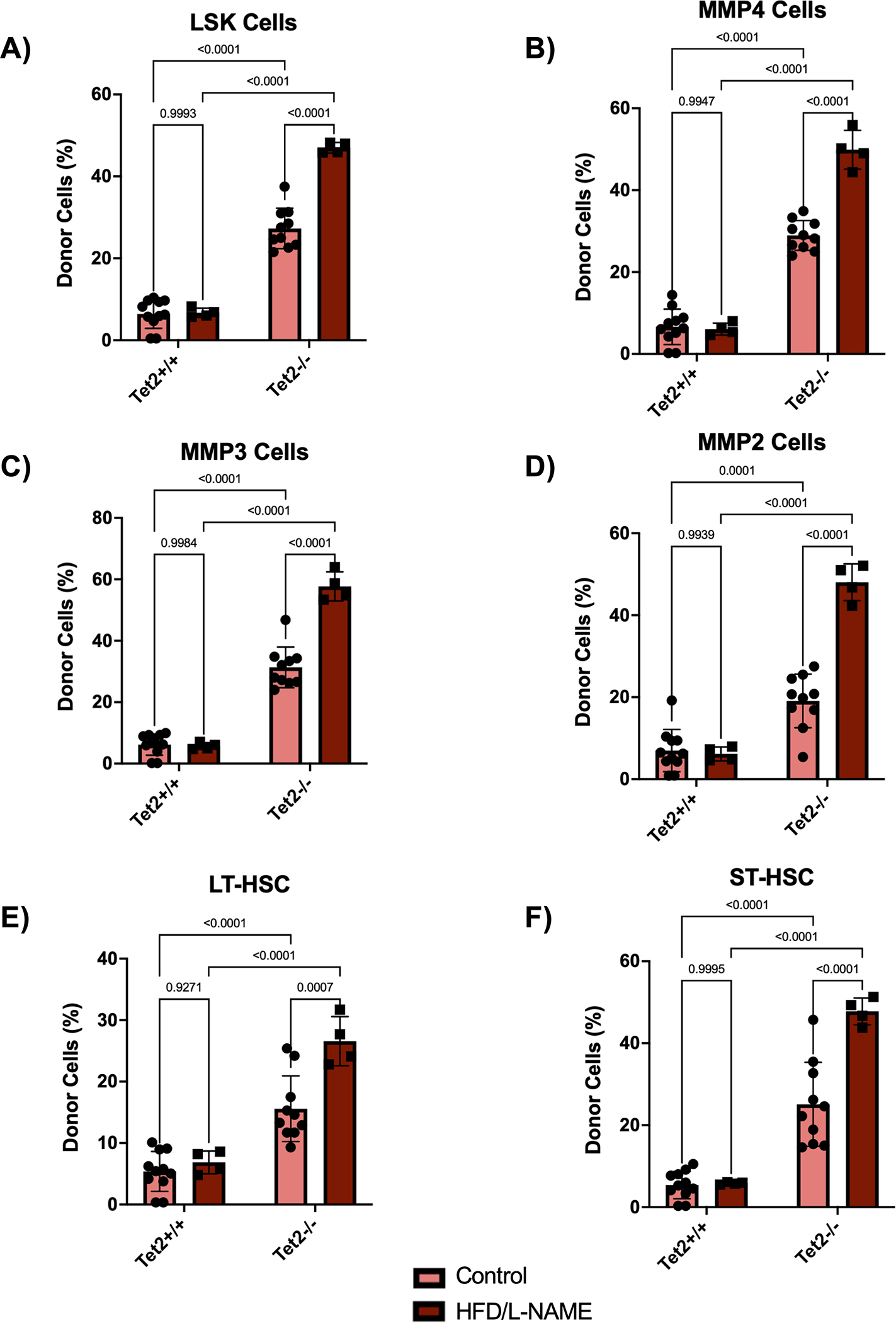
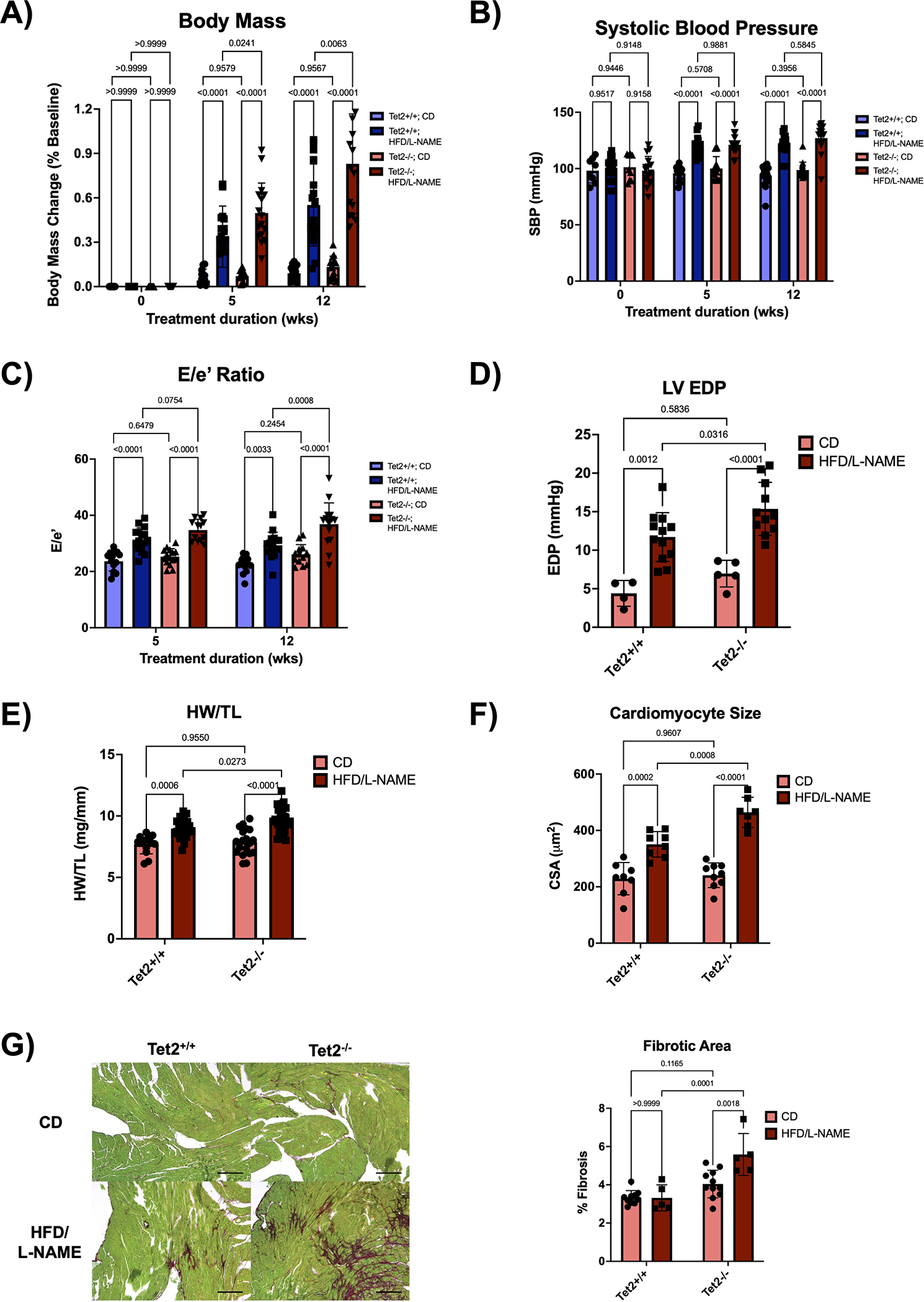
Results: Compared with controls, there was an enrichment of TET2-mediated CH in the HFpEF patient cohort (12% versus 0%, respectively; P=0.02). In the HFpEF cohort, patients with CH exhibited exacerbated diastolic dysfunction in terms of E/e' (14.9 versus 11.7, respectively; P=0.0096) and E/A (1.69 versus 0.89, respectively; P=0.0206) compared with those without CH. The association of CH with exacerbated diastolic dysfunction was corroborated in a validation cohort of individuals with HFpEF. In accordance, patients with HFpEF, an age ≥70 years, and CH exhibited worse prognosis in terms of 5-year cardiovascular-related hospitalization rate (hazard ratio, 5.06; P=0.042) compared with patients with HFpEF and an age ≥70 years without CH. To investigate the causal role of CH in HFpEF, nonconditioned mice underwent adoptive transfer with Tet2-wild-type or Tet2-deficient bone marrow and were subsequently subjected to a high-fat diet/L-NAME (Nω-nitro-l-arginine methyl ester) combination treatment to induce features of HFpEF. This model of Tet2-CH exacerbated cardiac hypertrophy by heart weight/tibia length and cardiomyocyte size, diastolic dysfunction by E/e' and left ventricular end-diastolic pressure, and cardiac fibrosis compared with the Tet2-wild-type condition.
Conclusions: CH is associated with worse heart function and prognosis in patients with HFpEF, and a murine experimental model of Tet2-mediated CH displays greater features of HFpEF.
Keywords: biomarkers; clonal hematopoiesis; heart failure; prognosis.
Conflict of interest statement
Figures
References
-
- Reddy YN, Borlaug BA. Heart Failure With Preserved Ejection Fraction. Curr Probl Cardiol. 2016;41:145–188. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Pandey A, Omar W, Ayers C, LaMonte M, Klein L, Allen NB, Kuller LH, Greenland P, Eaton CB, Gottdiener JS, et al. Sex and Race Differences in Lifetime Risk of Heart Failure With Preserved Ejection Fraction and Heart Failure With Reduced Ejection Fraction. Circulation. 2018;137:1814–1823. - PMC - PubMed
-
- Paulus WJ. Unfolding Discoveries in Heart Failure. N Engl J Med. 2020;382:679–682. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
