

Arginine Vasopressin Plays a Role in Microvascular Dysfunction After ST-Elevation Myocardial Infarction
- PMID: 37681545
- PMCID: PMC10547306
- DOI: 10.1161/JAHA.123.030473
Arginine Vasopressin Plays a Role in Microvascular Dysfunction After ST-Elevation Myocardial Infarction
Abstract
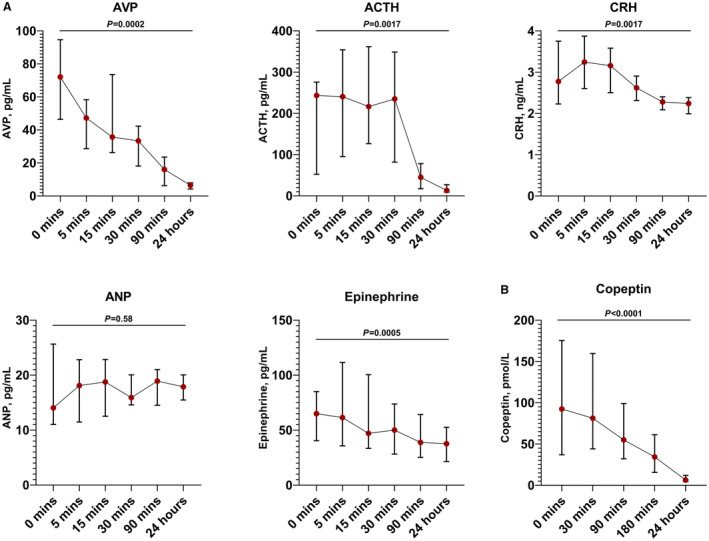
Background Coronary microvascular dysfunction (CMD) predicts mortality after ST-elevation-myocardial infarction (STEMI). Arginine vasopressin (AVP) may be implicated, but data in humans are lacking, and no study has investigated the link between arginine vasopressin and invasive measures of CMD. Methods and Results We invasively assessed CMD in 55 patients with STEMI treated with primary percutaneous coronary intervention (PPCI), by measuring the index of microcirculatory resistance after PPCI. In a separate group of 45 patients with STEMI/PPCI, recruited for a clinical trial, we measured infarct size and microvascular obstruction with cardiac magnetic resonance (CMR) imaging at 1 week and 12 weeks post-STEMI. Serum copeptin was measured at 4 time points before and after PPCI in all patients with STEMI. Plasma copeptin levels fell from 92.5 pmol/L before reperfusion to 6.4 pmol/L at 24 hours. Copeptin inversely correlated with diastolic, but not systolic, blood pressure (r=-0.431, P=0.001), suggesting it is released in response to myocardial ischemia. Persistently raised copeptin at 24 hours was correlated with higher index of microcirculatory resistance (r=0.372, P=0.011). Patients with microvascular obstruction on early CMR imaging showed a trend toward higher admission copeptin, which was not statistically significant. Copeptin levels were not associated with infarct size on either early or late CMR. Conclusions Patients with CMD after STEMI have persistently elevated copeptin at 24 hours, suggesting arginine vasopressin may contribute to microvascular dysfunction. Arginine vasopressin receptor antagonists may represent a novel therapeutic option in patients with STEMI and CMD.
Keywords: acute myocardial infarction; copeptin; microvascular dysfunction; microvascular obstruction.
Figures


References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli‐Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation. Eur Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Lawton JS, Tamis‐Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, Bittl JA, Cohen MG, DiMaio JM, Don CW, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e18–e114. doi: 10.1161/CIR.0000000000001038 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
