

Use of the Wearable Cardioverter-Defibrillator Among Patients With Myocarditis and Reduced Ejection Fraction or Ventricular Tachyarrhythmia: Data From a Multicenter Registry
- PMID: 37681569
- PMCID: PMC10547297
- DOI: 10.1161/JAHA.123.030615
Use of the Wearable Cardioverter-Defibrillator Among Patients With Myocarditis and Reduced Ejection Fraction or Ventricular Tachyarrhythmia: Data From a Multicenter Registry
Abstract
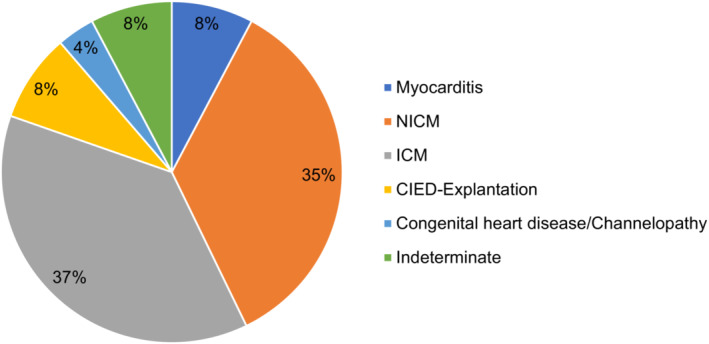
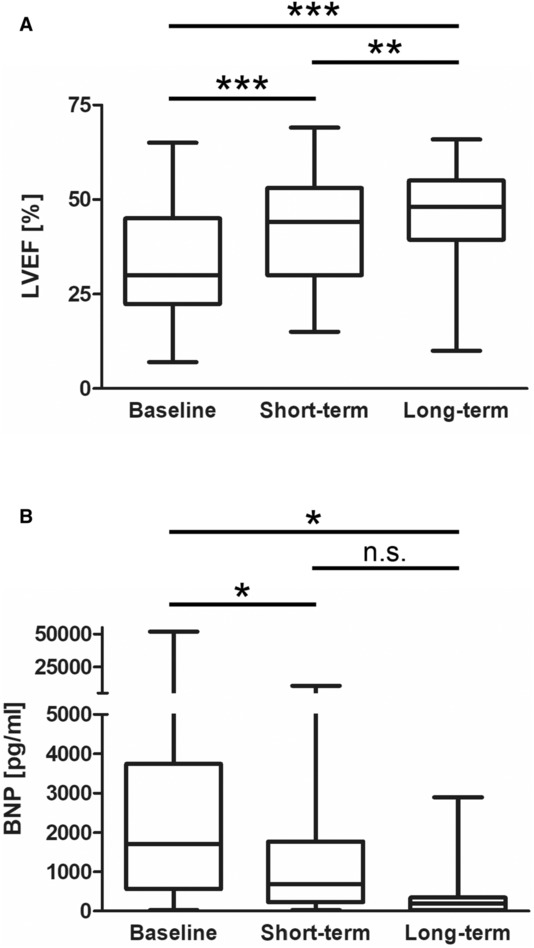
Background Data on the use of the wearable cardioverter-defibrillator (WCD) among patients with myocarditis remain sparse. Consequently, evidence for guideline recommendations in this patient population is lacking. Methods and Results In total, 1596 consecutive patients were included in a multicenter registry from 8 European centers, with 124 patients (8%) having received the WCD due to myocarditis and reduced left ventricular ejection fraction or prior ventricular tachyarrhythmia. The mean age was 51.6±16.3 years, with 74% being male. Patients were discharged after index hospitalization on heart failure medication: Angiotensin-converting enzyme inhibitors (62.5%), angiotensin-receptor-neprilysin inhibitor (22.9%), aldosterone-antagonists (51%), or beta blockers (91.4%). The initial median left ventricular ejection fraction was 30% (22%-45%) and increased to 48% (39%-55%) over long-term follow-up (P<0.001). The median BNP (brain natriuretic peptide) level at baseline was 1702 pg/mL (565-3748) and decreased to 188 pg/mL (26-348) over long-term follow-up (P=0.022). The mean wear time was 79.7±52.1 days and 21.0±4.9 hours per day. Arrhythmic event rates documented by the WCD were 9.7% for nonsustained ventricular tachycardia, 6.5% for sustained ventricular tachycardia, and 0% for ventricular fibrillation. Subsequently, 2.4% of patients experienced an appropriate WCD shock. The rate of inappropriate WCD shocks was 0.8%. All 3 patients with appropriate WCD shock had experienced ventricular tachycardia/ventricular fibrillation before WCD prescription, with only 1 patient showing a left ventricular ejection fraction <35%. Conclusions Patients with myocarditis and risk for occurrence of ventricular tachyarrhythmia may benefit from WCD use. Prior ventricular arrhythmia might appear as a better risk predictor than a reduced left ventricular ejection fraction <35% in this population.
Keywords: myocarditis; sudden cardiac death; ventricular tachycardia; wearable cardioverter‐defibrillator.
Figures
References
-
- Kragholm KH, Lindgren FL, Zaremba T, Freeman P, Andersen NH, Riahi S, Pareek M, Køber L, Torp‐Pedersen C, Søgaard P, et al. Mortality and ventricular arrhythmia after acute myocarditis: a nationwide registry‐based follow‐up study. Open Heart. 2021;8:e001806. doi: 10.1136/openhrt-2021-001806 - DOI - PMC - PubMed
-
- Zeppenfeld K, Tfelt‐Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, Charron P, Corrado D, Dagres N, Chillou C, et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43:3997–4126. doi: 10.1093/eurheartj/ehac262 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
