

Severe complications in the induction phase of therapy in a pediatric patient with T-cell acute lymphoblastic leukemia: A case report
- PMID: 37682188
- PMCID: PMC10489477
- DOI: 10.1097/MD.0000000000034965
Severe complications in the induction phase of therapy in a pediatric patient with T-cell acute lymphoblastic leukemia: A case report
Abstract
Rationale: Acute lymphoblastic leukemia (ALL) represents approximately 1-quarter of all new cases of childhood cancer. Although overall survival following diagnosis has improved in recent years, the toxicity of chemotherapy remains a concern.
Patient concerns: We describe an 11-year-old male patient diagnosed with T-cell precursor ALL who developed compounded complications during the induction phase of chemotherapy. Patient was hospitalized in the Department of Pediatric Hematology, Oncology, and Transplantology of the Medical University of Lublin, Poland. The patient's induction therapy was started according to the AIEOP-BFM ALL 2017 protocol IAp (International Collaborative Treatment Protocol for Children and Adolescents with Acute Lymphoblastic Leukemia).
Diagnoses: Patient developed compounded complications such as cholecystitis, hepatotoxicity, pancreatitis and myelosuppression.
Interventions: The patient was treated with leukapheresis, received a broad-spectrum antibiotic, potassium supplementation and hepatoprotective treatment and laparotomy cholecystectomy.
Outcomes: In the available literature, there is a limited amount of similar clinical cases with multiple complications in pediatric patients with ALL. Toxicities cause delays in the treatment of the underlying disease.
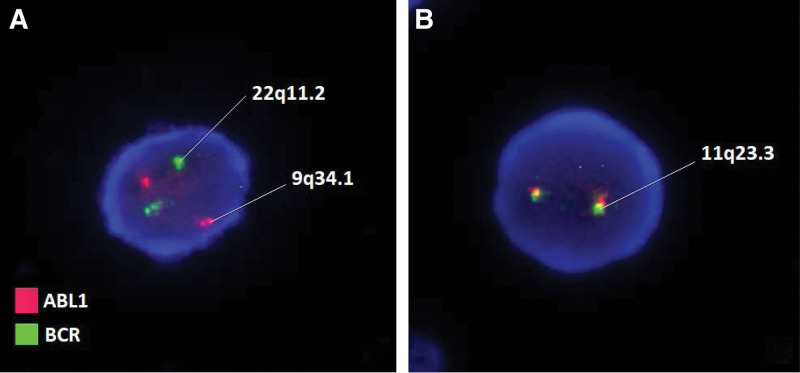
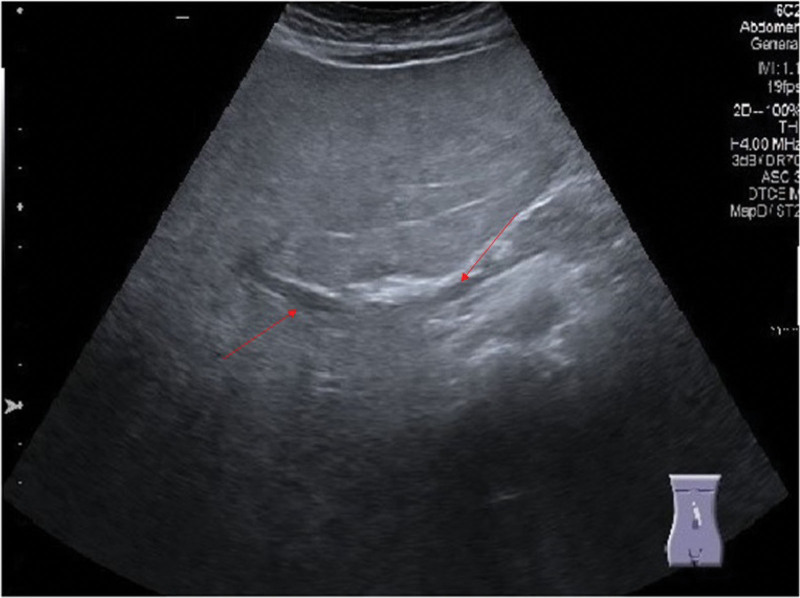
Lessons: In children with acute lymphoblastic leukemia, there are side effects during the treatment such as cholecystitis and pancreatitis. Complications during treatment require a quick response and modification of disease management. Abdominal ultrasound performed before treatment makes it possible to observe the dynamics of lesions. Genetic mutation analysis could allow us to more precisely respond to the possible susceptibility to and appearance of complications after the use of a given chemotherapeutic agent.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures



Similar articles
-
Early T-cell precursor acute lymphoblastic leukaemia in children treated in AIEOP centres with AIEOP-BFM protocols: a retrospective analysis.Lancet Haematol. 2016 Feb;3(2):e80-6. doi: 10.1016/S2352-3026(15)00254-9. Epub 2016 Jan 26. Lancet Haematol. 2016. PMID: 26853647
-
Diagnostic difficulties of AH1N1 influenza infection in children with acute lymphoblastic leukemia: Two case reports.Medicine (Baltimore). 2020 Oct 23;99(43):e22790. doi: 10.1097/MD.0000000000022790. Medicine (Baltimore). 2020. PMID: 33120795 Free PMC article.
-
Nelarabine, intensive L-asparaginase, and protracted intrathecal therapy for newly diagnosed T-cell acute lymphoblastic leukaemia in children and young adults (ALL-T11): a nationwide, multicenter, phase 2 trial including randomisation in the very high-risk group.Lancet Haematol. 2023 Jun;10(6):e419-e432. doi: 10.1016/S2352-3026(23)00072-8. Epub 2023 May 8. Lancet Haematol. 2023. PMID: 37167992 Clinical Trial.
-
[Therapeutic strategies for childhood high-risk acute lymphoblastic leukemia].Beijing Da Xue Xue Bao Yi Xue Ban. 2013 Apr 18;45(2):327-32. Beijing Da Xue Xue Bao Yi Xue Ban. 2013. PMID: 23591360 Review. Chinese.
-
A new onset drug induced diabetes mellitus presenting with diabetic ketoacidosis in a child undergoing treatment for B cell acute lymphoblastic leukemia. A case report and review of literature.J Pediatr Endocrinol Metab. 2024 Jan 29;37(4):367-370. doi: 10.1515/jpem-2023-0443. Print 2024 Apr 25. J Pediatr Endocrinol Metab. 2024. PMID: 38281148 Review.
References
-
- Surveillance, Epidemiology, and End Results Program: SEER Cancer Stat Facts: Childhood Leukemia (Ages 0–19). Bethesda, Md: National Cancer Institute, DCCPS, Surveillance Research Program. Available at: https://seer.cancer.gov/statfacts/html/childleuk.html. [access date 10, Dec 2022].
-
- Karrman K, Johansson B. Pediatric T-cell acute lymphoblastic leukemia. Genes Chromosomes Cancer. 2016;56:89–116. - PubMed
-
- Jayakrishnan TT, Groeschl RT, George B, et al. Management of acute cholecystitis in cancer patients: a comparative effectiveness approach. Surg Endosc. 2014;28:1505–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
