

SARS-CoV-2 Infection and Development of Islet Autoimmunity in Early Childhood
- PMID: 37682551
- PMCID: PMC10523173
- DOI: 10.1001/jama.2023.16348
SARS-CoV-2 Infection and Development of Islet Autoimmunity in Early Childhood
Abstract
Importance: The incidence of diabetes in childhood has increased during the COVID-19 pandemic. Elucidating whether SARS-CoV-2 infection is associated with islet autoimmunity, which precedes type 1 diabetes onset, is relevant to disease etiology and future childhood diabetes trends.
Objective: To determine whether there is a temporal relationship between SARS-CoV-2 infection and the development of islet autoimmunity in early childhood.
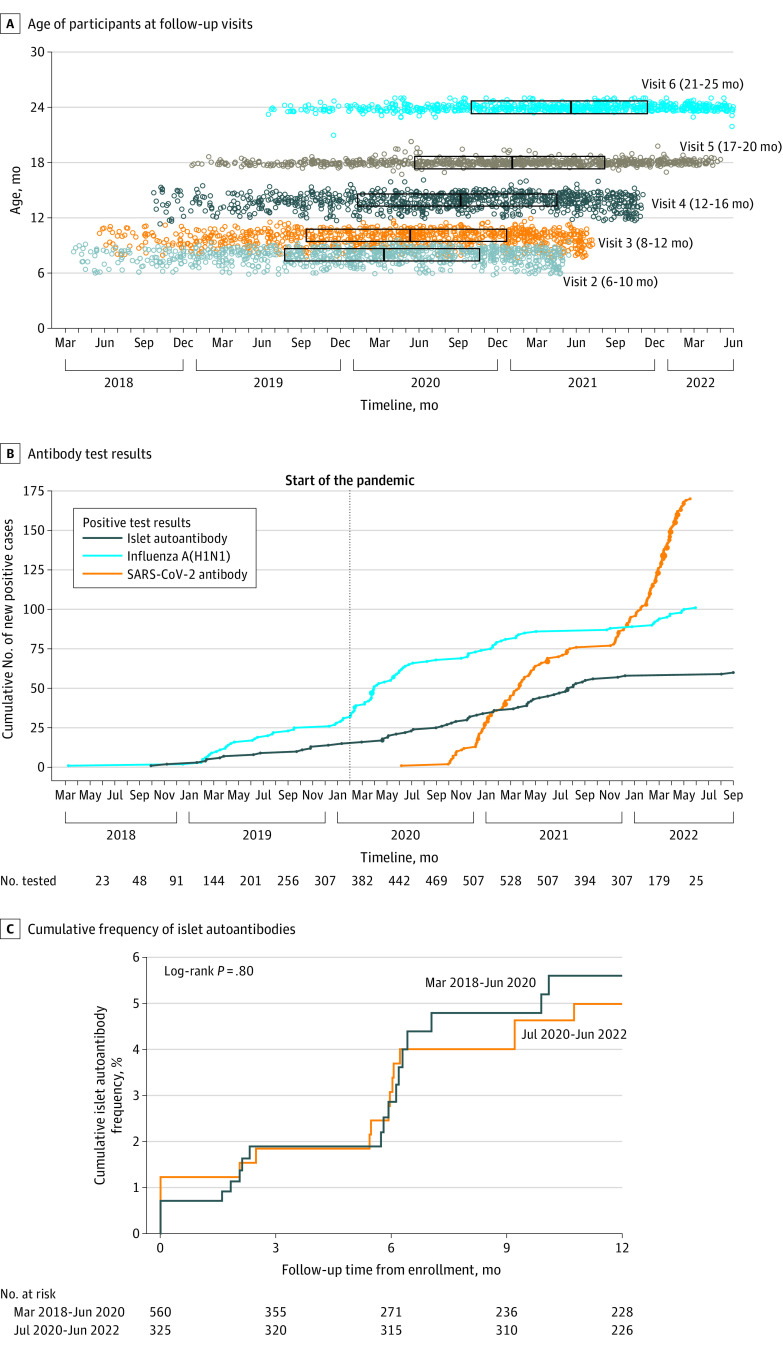
Design, setting, and participants: Between February 2018 and March 2021, the Primary Oral Insulin Trial, a European multicenter study, enrolled 1050 infants (517 girls) aged 4 to 7 months with a more than 10% genetically defined risk of type 1 diabetes. Children were followed up through September 2022.
Exposure: SARS-CoV-2 infection identified by SARS-CoV-2 antibody development in follow-up visits conducted at 2- to 6-month intervals until age 2 years from April 2018 through June 2022.
Main outcomes and measures: The development of multiple (≥2) islet autoantibodies in follow-up in consecutive samples or single islet antibodies and type 1 diabetes. Antibody incidence rates and risk of developing islet autoantibodies were analyzed.
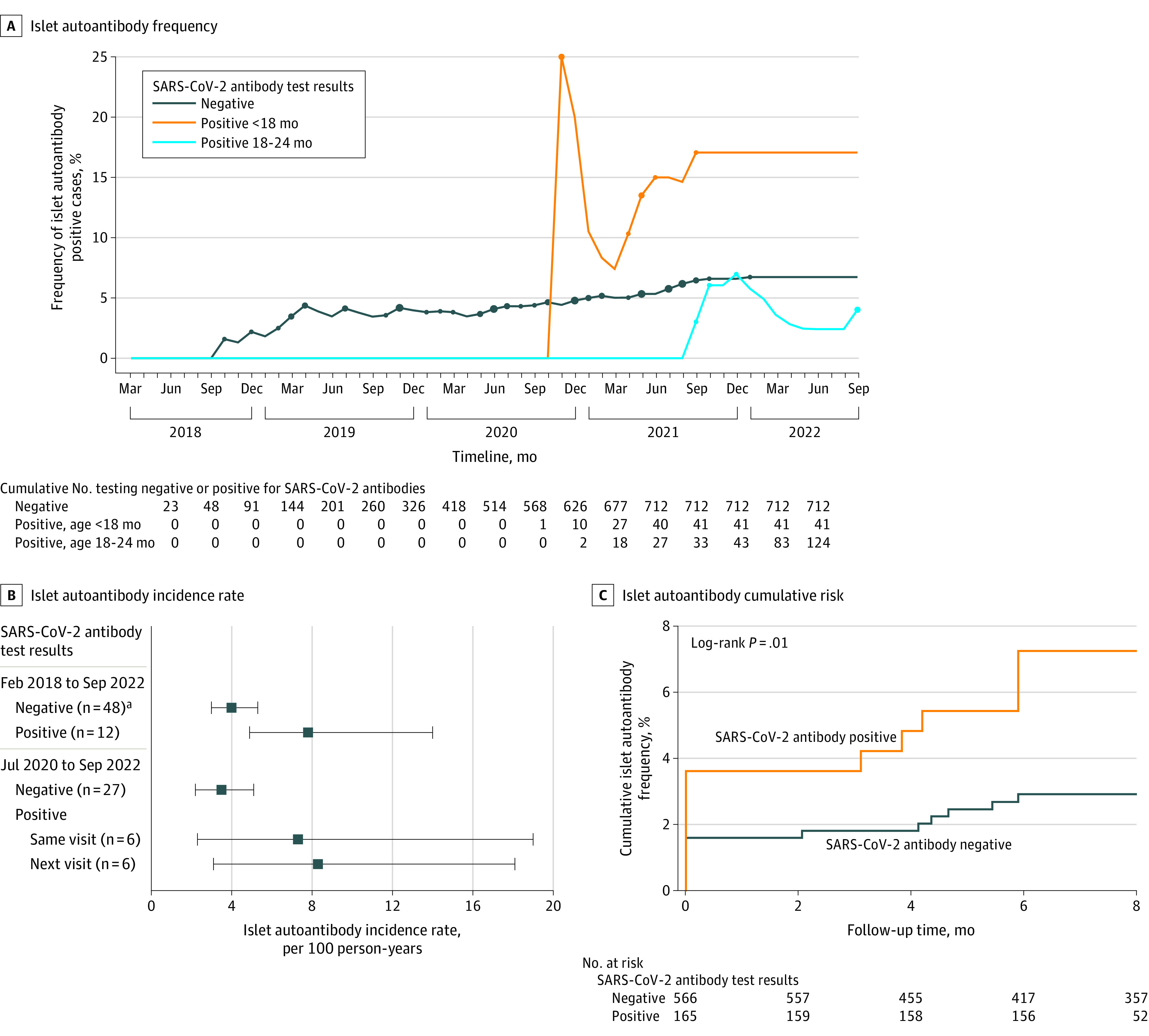
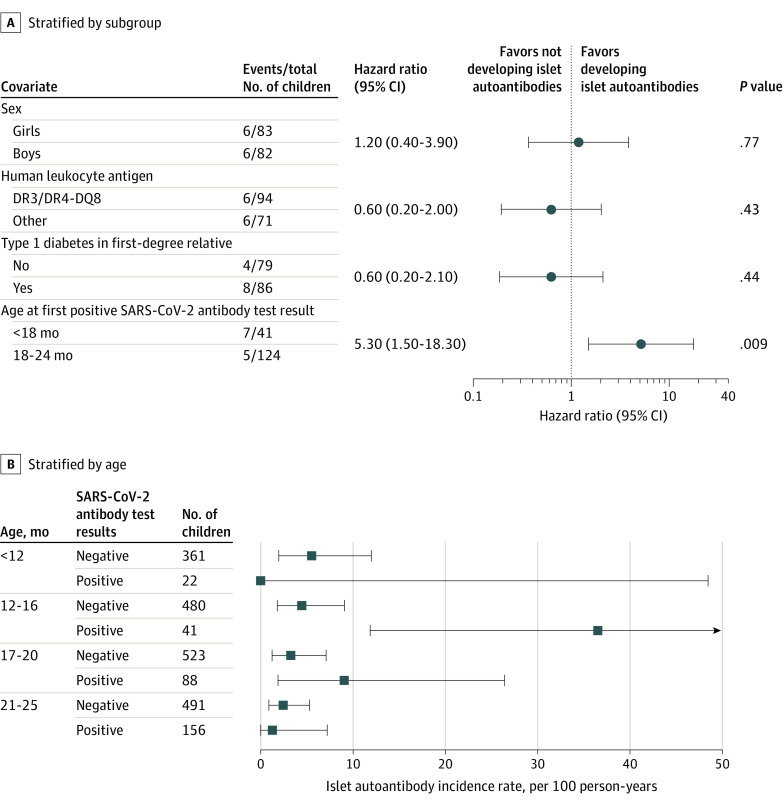
Results: Consent was obtained for 885 (441 girls) children who were included in follow-up antibody measurements from age 6 months. SARS-CoV-2 antibodies developed in 170 children at a median age of 18 months (range, 6-25 months). Islet autoantibodies developed in 60 children. Six of these children tested positive for islet autoantibodies at the same time as they tested positive for SARS-CoV-2 antibodies and 6 at the visit after having tested positive for SARS-CoV-2 antibodies. The sex-, age-, and country-adjusted hazard ratio for developing islet autoantibodies when the children tested positive for SARS-CoV-2 antibodies was 3.5 (95% CI, 1.6-7.7; P = .002). The incidence rate of islet autoantibodies was 3.5 (95% CI, 2.2-5.1) per 100 person-years in children without SARS-CoV-2 antibodies and 7.8 (95% CI, 5.3-19.0) per 100 person-years in children with SARS-CoV-2 antibodies (P = .02). Islet autoantibody risk in children with SARS-CoV-2 antibodies was associated with younger age (<18 months) of SARS-CoV-2 antibody development (HR, 5.3; 95% CI, 1.5-18.3; P = .009).
Conclusion and relevance: In young children with high genetic risk of type 1 diabetes, SARS-CoV-2 infection was temporally associated with the development of islet autoantibodies.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
