

Real-world ANASTASE study of atezolizumab+nab-paclitaxel as first-line treatment of PD-L1-positive metastatic triple-negative breast cancer
- PMID: 37684252
- PMCID: PMC10491680
- DOI: 10.1038/s41523-023-00579-2
Real-world ANASTASE study of atezolizumab+nab-paclitaxel as first-line treatment of PD-L1-positive metastatic triple-negative breast cancer
Erratum in
-
Author Correction: Real-world ANASTASE study of atezolizumab+nab-paclitaxel as first-line treatment of PD-L1-positive metastatic triple-negative breast cancer.NPJ Breast Cancer. 2023 Oct 30;9(1):89. doi: 10.1038/s41523-023-00596-1. NPJ Breast Cancer. 2023. PMID: 37903774 Free PMC article. No abstract available.
-
Author Correction: Real-world ANASTASE study of atezolizumab+nab-paclitaxel as first-line treatment of PD-L1-positive metastatic triple-negative breast cancer.NPJ Breast Cancer. 2024 Feb 5;10(1):13. doi: 10.1038/s41523-024-00619-5. NPJ Breast Cancer. 2024. PMID: 38316819 Free PMC article. No abstract available.
Abstract
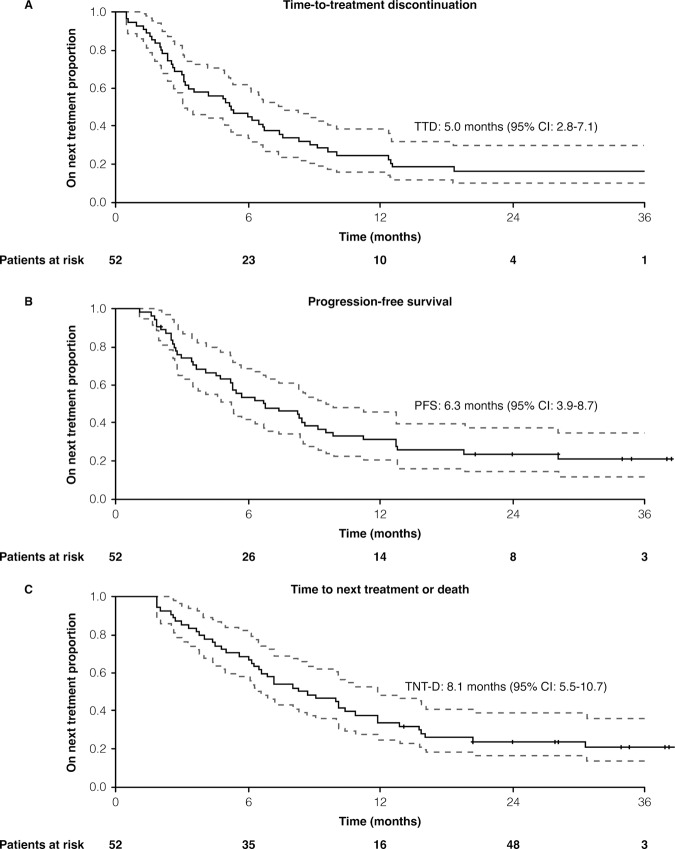
The combination of atezolizumab and nab-paclitaxel is recommended in the EU as first-line treatment for PD-L1-positive metastatic triple-negative breast cancer (mTNBC), based on the results of phase III IMpassion130 trial. However, 'real-world' data on this combination are limited. The ANASTASE study (NCT05609903) collected data on atezolizumab plus nab-paclitaxel in PD-L1-positive mTNBC patients enrolled in the Italian Compassionate Use Program. A retrospective analysis was conducted in 29 Italian oncology centers among patients who completed at least one cycle of treatment. Data from 52 patients were gathered. Among them, 21.1% presented de novo stage IV; 78.8% previously received (neo)adjuvant treatment; 55.8% patients had only one site of metastasis; median number of treatment cycles was five (IQR: 3-8); objective response rate was 42.3% (95% CI: 28.9-55.7%). The median time-to-treatment discontinuation was 5 months (95% CI: 2.8-7.1); clinical benefit at 12 months was 45.8%. The median duration of response was 12.7 months (95% CI: 4.1-21.4). At a median follow-up of 20 months, the median progression-free survival was 6.3 months (95% CI: 3.9-8.7) and the median time to next treatment or death was 8.1 months (95% CI: 5.5-10.7). At 12 months and 24 months, the overall survival rates were 66.3% and 49.1%, respectively. The most common immune-related adverse events included rash (23.1%), hepatitis (11.5%), thyroiditis (11.5%) and pneumonia (9.6%). Within the ANASTASE study, patients with PD-L1-positive mTNBC treated with first-line atezolizumab plus nab-paclitaxel achieved PFS and ORR similar to those reported in the IMpassion130 study, with no unexpected adverse events.
© 2023. Springer Nature Limited.
Conflict of interest statement
The Authors declare no competing interests.
Figures
References
-
- Garrido-Castro AC, Lin NU, Polyak K. Insights into molecular classifications of triple-negative breast cancer: improving patient selection for treatment. Cancer Discov. 2019;9:176–198. doi: 10.1158/2159-8290.CD-18-1177. - DOI - PMC - PubMed
