

Electrocardiographic Markers of Adverse Left Ventricular Remodeling and Myocardial Fibrosis in Severe Aortic Stenosis
- PMID: 37685655
- PMCID: PMC10488170
- DOI: 10.3390/jcm12175588
Electrocardiographic Markers of Adverse Left Ventricular Remodeling and Myocardial Fibrosis in Severe Aortic Stenosis
Abstract
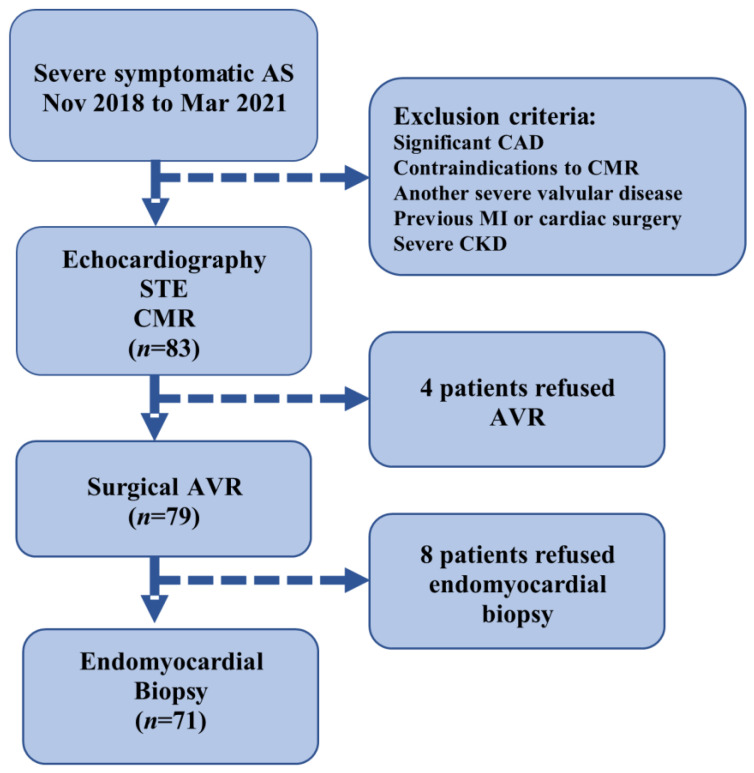
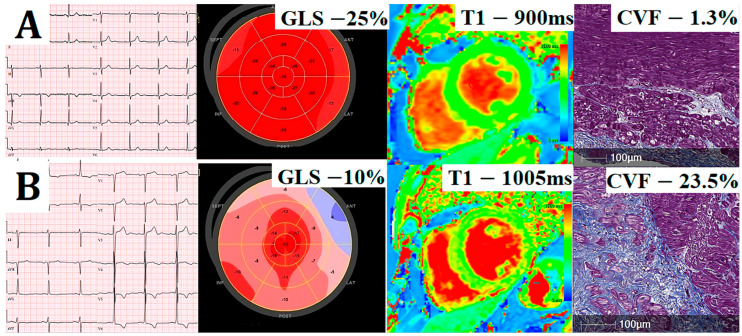
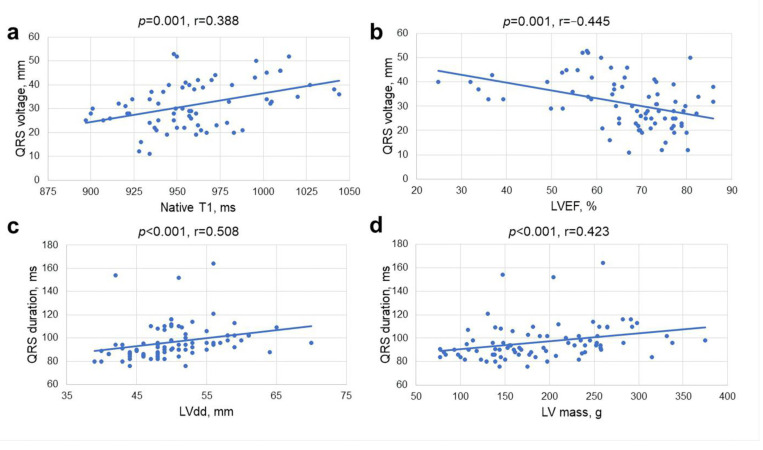
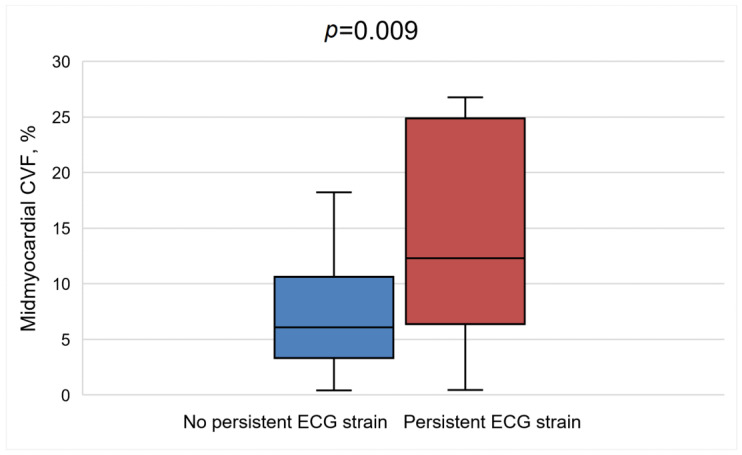
The optimal timing for aortic valve replacement (AVR) in aortic stenosis (AS) is still controversial and may be guided by markers of adverse left ventricular (LV) remodeling. We aim to assess electrocardiographic (ECG) strain in relation to LV remodeling and myocardial fibrosis. 83 severe AS patients underwent surgical AVR, with preoperative 12-lead ECG, cardiovascular magnetic resonance with T1 mapping and echocardiography with global longitudinal strain analysis. Collagen volume fraction (CVF) was measured in myocardial biopsies sampled during AVR. Patients with ECG strain had more severe AS, more advanced LV remodeling and evidence of heart failure. Patients with ECG strain had more diffuse fibrosis, as evident by higher mean native T1 values (974.8 ± 34 ms vs. 946.5 ± 28 ms, p < 0.001). ECG strain was the only predictor of increased LV mass index on multivariate regression analysis (OR = 7.10, 95% CI 1.46-34.48, p = 0.02). Patients with persistent ECG strain at 1 year following AVR had more advanced LV remodeling and more histological fibrosis (CVF 12.5% vs. 7.3%, p = 0.009) at baseline assessment. Therefore, ECG strain is a marker of adverse LV remodeling and interstitial myocardial fibrosis. Lack of improvement in ECG strain following AVR indicates more advanced baseline LV injury and higher levels of myocardial fibrosis.
Keywords: T1 mapping; aortic stenosis; cardiovascular magnetic resonance; electrocardiographic strain; myocardial fibrosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Dweck M.R., Joshi S., Murigu T., Gulati A., Alpendurada F., Jabbour A., Maceira A., Roussin I., Northridge D.B., Kilner P.J., et al. Left ventricular remodeling and hypertrophy in patients with aortic stenosis: Insights from cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012;14:50. doi: 10.1186/1532-429X-14-50. - DOI - PMC - PubMed
-
- Everett R.J., Tastet L., Clavel M.-A., Chin C.W., Capoulade R., Vassiliou V.S., Kwiecinski J., Gomez M., van Beek E.J., White A.C., et al. Progression of Hypertrophy and Myocardial Fibrosis in Aortic Stenosis: A Multicenter Cardiac Magnetic Resonance Study. Circ. Cardiovasc. Imaging. 2018;11:e007451. doi: 10.1161/CIRCIMAGING.117.007451. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
