

Analysis of P(v-a)CO2/C(a-v)O2 Ratio and Other Perfusion Markers in a Population of 98 Pediatric Patients Undergoing Cardiac Surgery
- PMID: 37685767
- PMCID: PMC10488867
- DOI: 10.3390/jcm12175700
Analysis of P(v-a)CO2/C(a-v)O2 Ratio and Other Perfusion Markers in a Population of 98 Pediatric Patients Undergoing Cardiac Surgery
Abstract
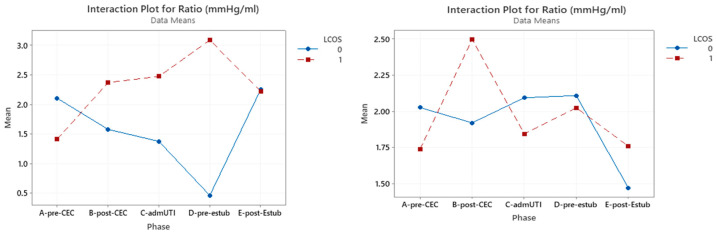
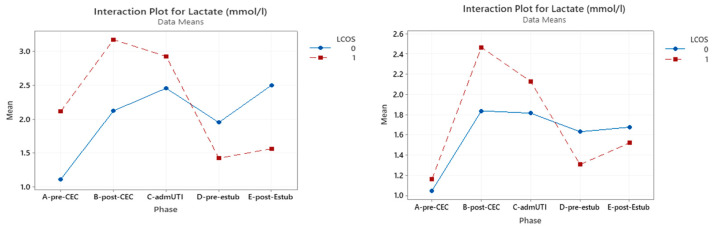
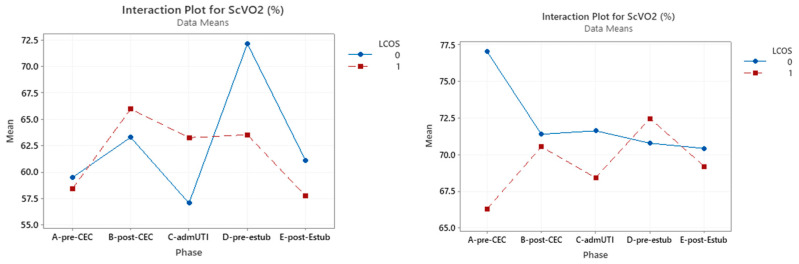
Background: The so-called Low Cardiac Output Syndrome (LCOS) is one of the most common complications in pediatric patients with congenital heart disease undergoing corrective surgery. LCOS requires high concentrations of inotropes to support cardiac contractility and improve cardiac output, allowing for better systemic perfusion. To date, serum lactate concentrations and central venous oxygen saturation (ScVO2) are the most commonly used perfusion markers, but they are not completely reliable in identifying a state of global tissue hypoxia. The study aims to evaluate whether the venoarterial carbon dioxide difference/arterial-venous oxygen difference ratio [P(v-a)CO2/C(a-v)O2] can be a good index to predict the development of LCOS in the aforementioned patients, so as to treat it promptly.
Methods: This study followed a population of 98 children undergoing corrective cardiac surgery from June 2018 to October 2020 at the Department of Cardiac Surgery of University Hospital Integrated Trust and their subsequent admission at the Postoperative Cardiothoracic Surgery Intensive Care Unit. During the study, central arterial and venous blood gas analyses were carried out before and after cardiopulmonary bypass (CPB) (pre-CPB and post-CPB), at admission to the intensive care unit, before and after extubation, and at any time of instability or modification of the patient's clinical and therapeutic conditions.
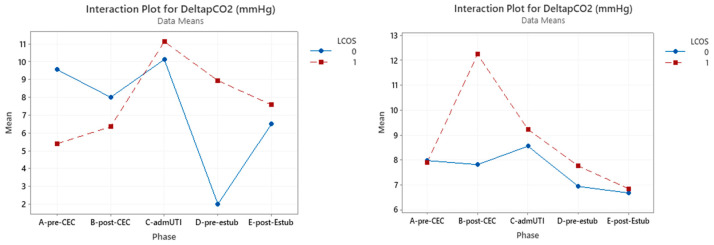
Results: The data analysis shows that 46.9% of the children developed LCOS (in line with the current literature) but that there is no statistically significant association between the P(v-a)CO2/C(a-v)O2 ratio and LCOS onset. Despite the limits of statistical significance, however, a 31% increase in the ratio emerged from the pre-CPB phase to the post-CPB phase when LCOS is present.
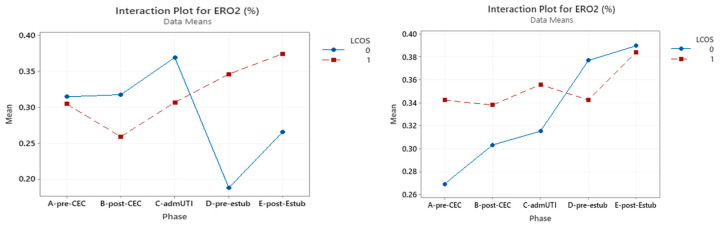
Conclusions: This study confirms a statistically significant association between the most used markers in adult patients (serum lactate concentration, ScVO2, and oxygen extraction ratio-ERO2) measured in the pre-CPB phase and the incidence of LCOS onset, especially in patients with hemodynamic instability before surgery.
Keywords: cardiopulmonary bypass; congenital heart disease; infant; physiologic monitoring; postoperative care; venoarterial carbon dioxide difference.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Rihal C.S., Naidu S.S., Givertz M.M., Szeto W.Y., Burke J.A., Kapur N.K., Kern M., Garratt K.N., Goldstein J.A., Dimas V., et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care: Endorsed by the American Heart Assocation, the Cardiological Society of India, and Sociedad Latino Americana de Cardiologia Intervencion; Affirmation of Value by the Canadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d’intervention. J. Am. Coll. Cardiol. 2015;65:e7–e26. doi: 10.1016/j.jacc.2015.03.036. - DOI - PubMed
-
- Johnson W.H. Pediatric Cardiology: The Essential Pocket Guide. 3rd ed. John Wiley and Sons; Hoboken, NJ, USA: 2014.
LinkOut - more resources
Full Text Sources
