

Acute-Onset Retinal Conditions Mimicking Acute Optic Neuritis: Overview and Differential Diagnosis
- PMID: 37685787
- PMCID: PMC10488521
- DOI: 10.3390/jcm12175720
Acute-Onset Retinal Conditions Mimicking Acute Optic Neuritis: Overview and Differential Diagnosis
Abstract
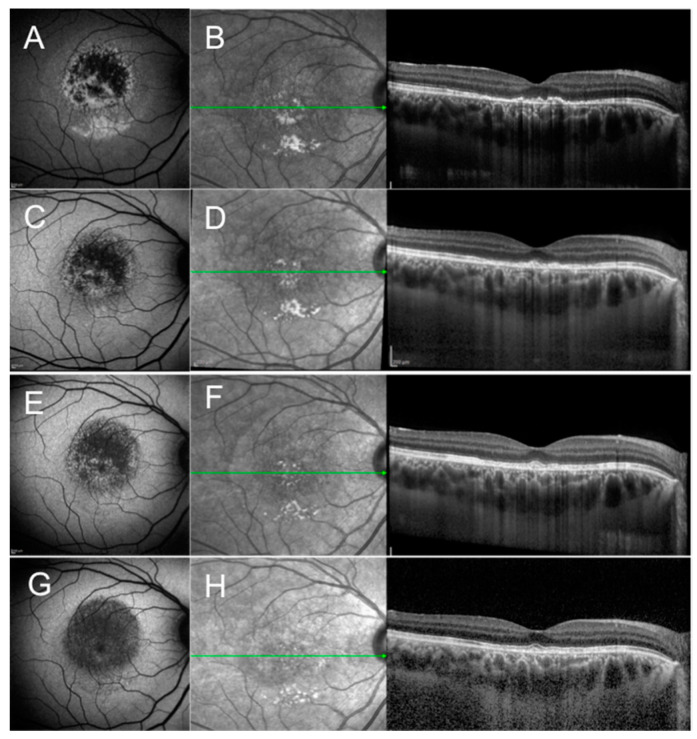
Acute optic neuritis (AON) is a common cause of sudden visual loss in young patients. Because of the risk of demyelinating disease, patients affected by unilateral or bilateral optic neuritis should be evaluated and treated accordingly. Despite advancements in imaging of the brain and retina, misdiagnosis of AON is not uncommon. Indeed, some acute disorders of the retina have the potential to mimic AON and their prompt diagnosis may avoid unnecessary neurologic investigation, psychological stress to the patient, and delays in treatment. This review describes uncommon retinal disorders presenting with sudden-onset visual loss and absent or subtle funduscopic manifestation that can mimic AON. Multimodal retinal imaging is essential in detecting these conditions and in their differential diagnosis. It behooves neurologists and general ophthalmologists to be aware of these entities and be familiar with multimodal imaging of the retina.
Keywords: acute-onset visual loss; differential diagnosis; multimodal imaging; optic neuritis; retinal conditions.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- Shindo A., Kokubo Y., Taniguchi A., Kuze M., Kuzuhara S. Case of acute zonal occult outer retinopathy (AZOOR): A 15 years’ mislabeling as retrobulbar optic neuritis. Rinsho Shinkeigaku. 2007;47:116–118. - PubMed
-
- Freund K.B., Yannuzzi L.A., Barile G.R., Spaide R.F., Milewski S.A., Guyer D.R. The expanding clinical spectrum of unilateral acute idiopathic maculopathy. Arch. Ophthalmol. 1996;114:555–559. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
