

Ketone body 3-hydroxybutyrate elevates cardiac output through peripheral vasorelaxation and enhanced cardiac contractility
- PMID: 37688627
- PMCID: PMC10492777
- DOI: 10.1007/s00395-023-01008-y
Ketone body 3-hydroxybutyrate elevates cardiac output through peripheral vasorelaxation and enhanced cardiac contractility
Abstract
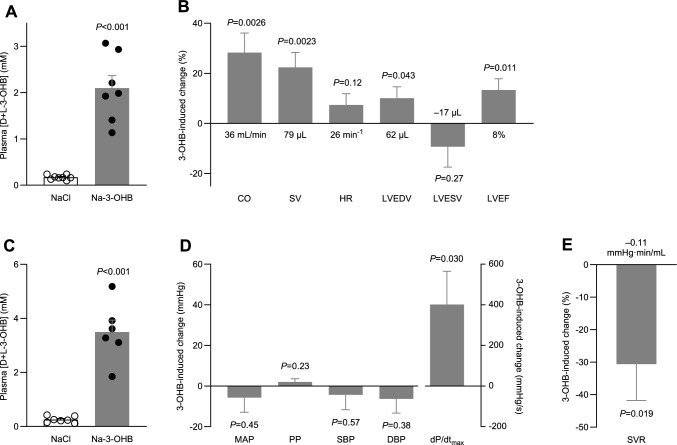
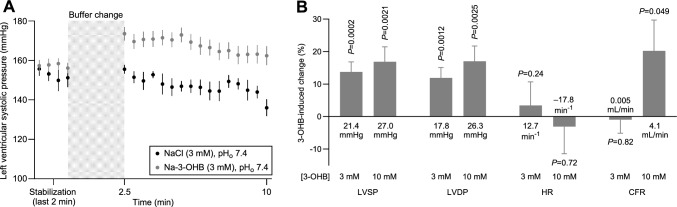
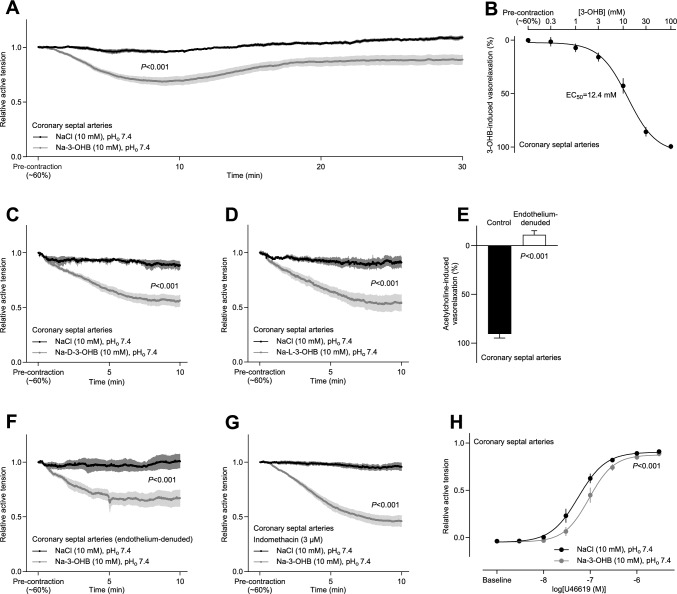
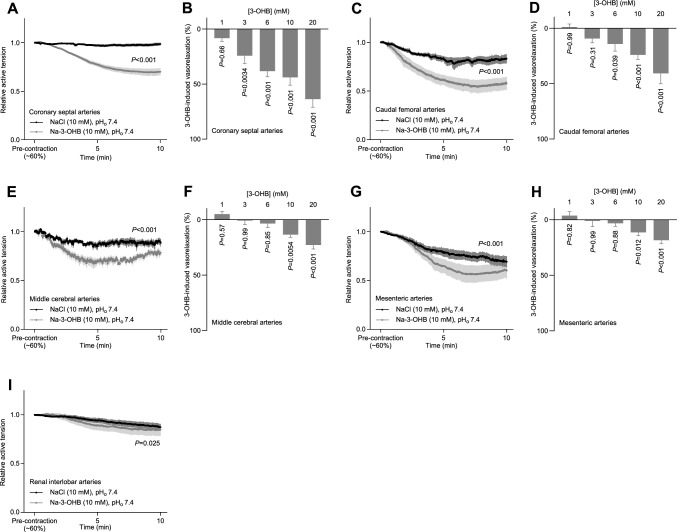
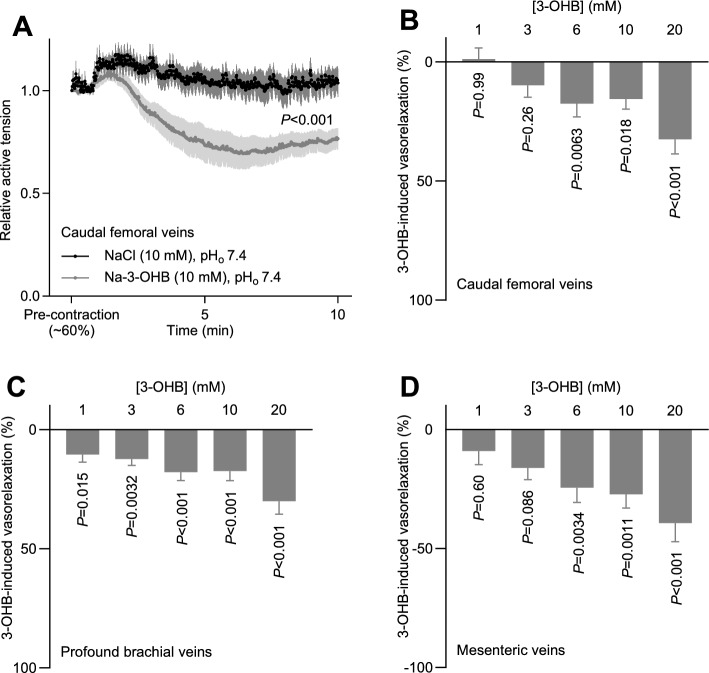
The ketone body 3-hydroxybutyrate (3-OHB) increases cardiac output and myocardial perfusion without affecting blood pressure in humans, but the cardiovascular sites of action remain obscure. Here, we test the hypothesis in rats that 3-OHB acts directly on the heart to increase cardiac contractility and directly on blood vessels to lower systemic vascular resistance. We investigate effects of 3-OHB on (a) in vivo hemodynamics using echocardiography and invasive blood pressure measurements, (b) isolated perfused hearts in Langendorff systems, and (c) isolated arteries and veins in isometric myographs. We compare Na-3-OHB to equimolar NaCl added to physiological buffers or injection solutions. At plasma concentrations of 2-4 mM in vivo, 3-OHB increases cardiac output (by 28.3±7.8%), stroke volume (by 22.4±6.0%), left ventricular ejection fraction (by 13.3±4.6%), and arterial dP/dtmax (by 31.9±11.2%) and lowers systemic vascular resistance (by 30.6±11.2%) without substantially affecting heart rate or blood pressure. Applied to isolated perfused hearts at 3-10 mM, 3-OHB increases left ventricular developed pressure by up to 26.3±7.4 mmHg and coronary perfusion by up to 20.2±9.5%. Beginning at 1-3 mM, 3-OHB relaxes isolated coronary (EC50=12.4 mM), cerebral, femoral, mesenteric, and renal arteries as well as brachial, femoral, and mesenteric veins by up to 60% of pre-contraction within the pathophysiological concentration range. Of the two enantiomers that constitute racemic 3-OHB, D-3-OHB dominates endogenously; but tested separately, the enantiomers induce similar vasorelaxation. We conclude that increased cardiac contractility and generalized systemic vasorelaxation can explain the elevated cardiac output during 3-OHB administration. These actions strengthen the therapeutic rationale for 3-OHB in heart failure management.
Keywords: 3-hydroxybutyrate; Contractile function; Enantiomers; Ketone bodies; Metabolism; Vasorelaxation.
© 2023. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Bedi KC, Jr, Snyder NW, Brandimarto J, Aziz M, Mesaros C, Worth AJ, Wang LL, Javaheri A, Blair IA, Margulies KB, Rame JE. Evidence for intramyocardial disruption of lipid metabolism and increased myocardial ketone utilization in advanced human heart failure. Circulation. 2016;133:706–716. doi: 10.1161/CIRCULATIONAHA.115.017545. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
